As with any educational or academic en devour, as soon as you finish a paper/poster/presentation, a new publication comes out that would have been awesome to include. I finished and published the Pneumonia podcast on July 12th and on July 14th, the IDSA/ATS released their updated guidelines on managing healthcare-associated (HAP) and ventilator-associated (VAP) pneumonia. Luckily, they didn’t change anything earth-shattering, just tightened them up a bit. Antibiotic regimens are below and they recommend 7-days total of therapy.
Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. American journal of respiratory and critical care medicine. 171(4):388-416. 2005. [pubmed]
File TM, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgraduate medicine. 122(2):130-41. 2010. [pubmed]
Almirall J, Bolíbar I, Balanzó X, González CA. Risk factors for community-acquired pneumonia in adults: a population-based case-control study. The European respiratory journal. 13(2):349-55. 1999. [pubmed]
Mandell LA, Wunderink RG, Anzueto A. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 44 Suppl 2:S27-72. 2007. [pubmed]
Musher DM, Thorner AR. Community-acquired pneumonia. The New England journal of medicine. 371(17):1619-28. 2014. [pubmed]
Jain S, Self WH, Wunderink RG. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. The New England journal of medicine. 373(5):415-27. 2015. [pubmed]
Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 278(17):1440-5. 1997. [pubmed]
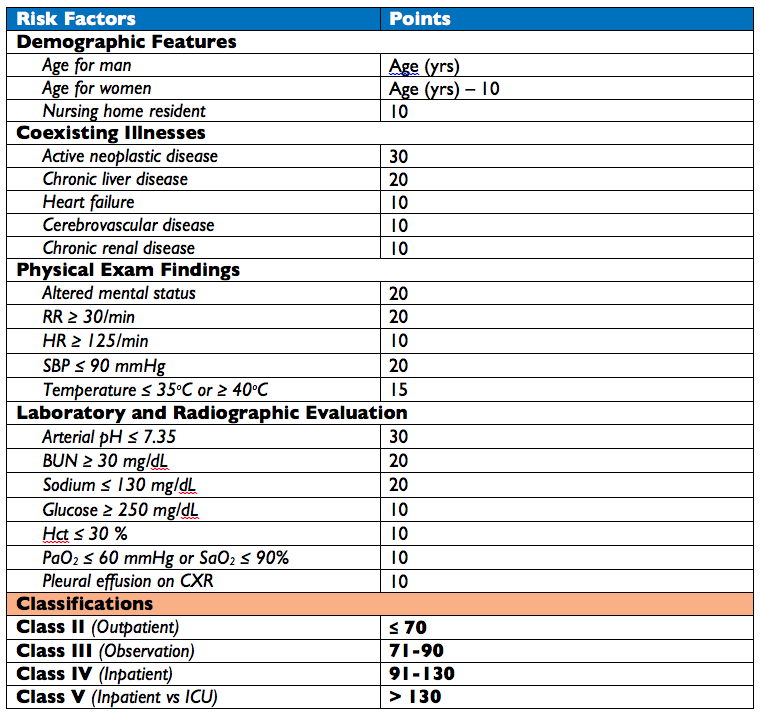
Fine MJ, Auble TE, Yealy DM. A prediction rule to identify low-risk patients with community-acquired pneumonia. The New England journal of medicine. 336(4):243-50. 1997. [pubmed]
Lim WS, van der Eerden MM, Laing R. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 58(5):377-82. 2003. [pubmed]
Charles PG, Wolfe R, Whitby M. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 47(3):375-84. 2008. [pubmed]
Pugh R, Grant C, Cooke RP, Dempsey G. Short-course versus prolonged-course antibiotic therapy for hospital-acquired pneumonia in critically ill adults. The Cochrane database of systematic reviews. 2015. [pubmed]
1st described in the late 1400s and 1st published in 1544 by Jean Fernal
1st appendectomy was performed in 1736 on an 11yo boy
233/100,000 population
May occur throughout life, but is most common age group is 10-19yo and slightly more common in men
Badass of the Millennium goes to….Leonid Rogozov. He was the only physician on a Soviet team in Antarctica in 1961 and performed an appendectomy…on himself…and survived (Article here)
Leonid Rogozov performing an appendectomy on himself – 1961
Anatomy of the Appendix
Wikipedia
Located where the taenia coli converge at the base of cecum
Average length 6-9cm, outer diameter 3-8mm, and luminal diameter 1-3mm
Arterial supply is from appendicular branch of the ileocolic artery
The attachment of the base of the appendix is constant, but the tip may be positioned:
Retrocecal (most common)
Subcecal
Preileal
Postileal
Pelvic
Wikipedia
Pathogenesis
Follows traditional predictable series of events for inflammation of a hollow visceral organ:
Inflammation
Most commonly by an obstruction
Fecalith, calculi, lymphoid hyperplasia, infection, mass
Causes a closed-loop obstruction
Distention
Normal secretion and bacterial overgrowth
Causes visceral nerve pain
Luminal pressure > perfusion
Involves the serosa
Causes parietal pain
Perforation
As areas of ischemia progress and pressures increase, perforation may occur
May be contained (localized) or cause peritonitis
Although this progression is predictable, the time frame may be variable
Perforation may occur anywhere from 24-48 hours after symptom onset
History
Abdominal pain occurs first
Starts as diffuse, periumbilical
Appendix position may alter pain location
Nausea and vomiting then follows
Anorexia (Negative Cheeseburger Sign)
Last is migratory pain to RLQ (50-60%)
Physical Examination
Often non-specific as appendix position, time course of illness, and patient anatomy may obscure findings
Classic physical exam findings include:
McBurney’s Point Tenderness
Maximal tenderness 3cm from ASIS, or 1/3rd the distance from ASIS to umbilicus
Rovsing’s Sign
Palpation or rebound pressure of LLQ causes RLQ pain
Psoas Sign (retrocecal)
Pain in RLQ when ipsilateral hip is extended or flexed against resistance
Obsturator Sign (pelvic)
Pain in RLQ with internal rotation of ipsilateral hip with flexed knee
Guarding and peritoneal signs may be seen with perforation
Laboratory Studies
CBC with differential and CRP are needed for the scoring systems, but are not very specific
Pretest Probability Scoring Systems
Alvarado Score
Developed in 1986 and modified in 1994
Appendicitis Inflammatory Response (AIR) Score
Developed in 2008
Pediatric Appendicitis Score
Developed in 2002
Interpretation
Alvarado Score
0-3 – low probability (discharge)
4-6 – indeterminate (image or admit)
≥ 7 – high probability (admit or surgery)
AIR Score
0-4 – Low probability (discharge)
5-8 – Indeterminate (image or admit)
≥ 9 – high probability (admit or surgery)
PAS
< 3 – low probability (discharge)
3-7 – indeterminate (image or admit)
≥ 8 – high probability (admit and consult)
Radiographic Imaging
Imaging is generally reserved for indeterminate cases or special populations (children, women, elderly) as clinical examination is just as effective as imaging in ruling-out appendicitis
Computed Tomography
IV contrast
Findings suggesting appendicitis:
≥ 6mm diameter
Appendiceal wall thickening ≥ 2mm
Periappendiceal fat stranding
Appendicolith
Ultrasound
Study of choice in children and pregnant women and becoming study of choice in adults
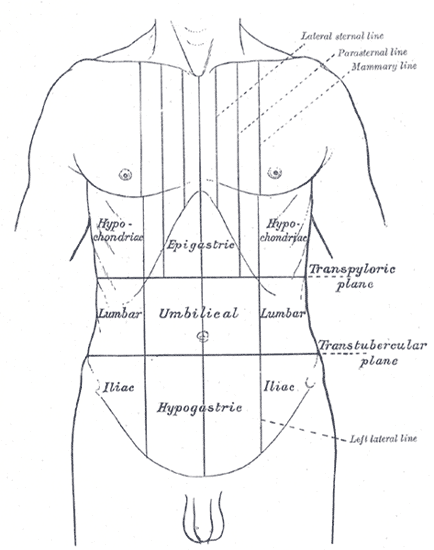
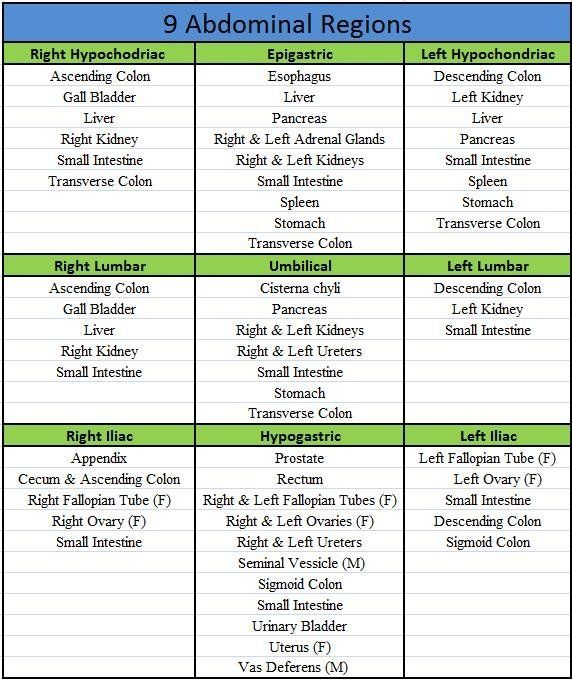
The lesser utilized dividing of the abdomen into 9 section is more academic than practical (though I would argue the more specific you can be in your documentation and conversation with consultants, the better). To better orient to these regions you have to be familiar with the following four anatomic lines: transpyloric line (Addison’s plane), transtubercular line, and the left and right mammary line.
Drawing these 4 lines make up the “tic-tac-toe” board of the abdomen and the nine regions of the abdomen:
Right hypochondriac
Epigastric
Left hypochondriac
Right lumbar
Umbilical
Left Lumbar
Right iliac
Hypogastric
Left iliac
So what structures are found in each region?
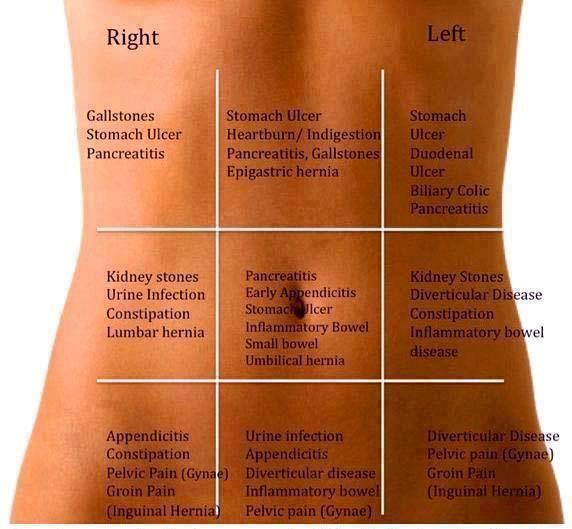
Now you know what organs are found in each section, what are some differential diagnoses for each region if a patient comes in with localized abdominal pain?
Question #1 – What are the muscles that make up the rotator cuff?
Answer – Supraspinatus, Infraspinatus, Teres Minor, and Subscapularis
Question #2 – What is AT LEAST one maneuver to assess each of these muscles
Keep in mind, there are several maneuvers of the shoulder and many overlap into other structures. These are the more common individual maneuvers that I think general practice PAs need to know.
Supraspinatus
Drop Arm test
Description – Patient is seated with examiner to the front. Examiner grasps the patient’s wrist and passively abducts the patient’s shoulder to 90 degrees. Examiner releases the patient’s arm with instructions to slowly lower the arm. Test is positive if the patient is unable to lower his or her arm in a smooth, controlled fashion
Infraspinatus
Dropping Sign
Description – The patient stands with the arm at the side with the elbow at 90 degrees and the humerus medially rotated to 45 degrees. Patient then resists external rotation. Pain or the inability to resist medial rotation indicates a positive test for an infraspinatus strain.
Teres Minor
Hornblower (Patte) Test
Description – Elevate the patient’s arm to 90 degrees in the scapular plane and then flex the elbow to 90 degrees, and the patient is asked to laterally rotate the shoulder. A positive test occurs with weakness and/or pain.
Subscapularis
Lift Off (Gerber) Test
Description – The patient stands and places the dorsum of the hand against mid-lumbar spine. The patient then lifts hand away from the back. An inability to perform this action indicates subscapularis weakness or injury.