47yo male presents to emergency department with a 3 day history of progressive abdominal pain, nausea, and vomiting. He reports the pain the as a constant, boring pain that radiates to his back. Eating seems to aggravate it and sitting up and leaning forward sometimes help. He does report occasional alcohol use. He reports subjective fever, but denies chills, recent illnesses, diarrhea, constipation, hematemesis, melena, or hematochezia. Vital signs show BP-112/80, HR-118, RR-22, O2-100%, and temperature 39oC (102.2oF). Physical exam reveals mild distension, generalized abdominal tenderness to deep palpation, absent bowel sounds, and the below finding:

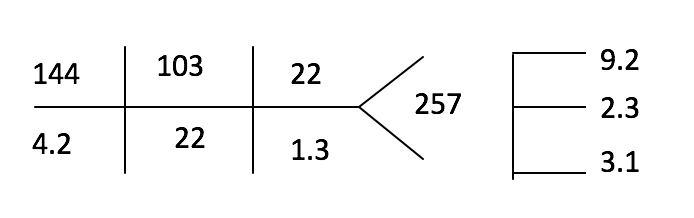
Laboratory studies are:


AST – 322U/L ALT – 45U/L ALP – 14U/L
LDH – 833U/L GGT – 15U/L Bilirubin – 1.9
Amylase – 209U/L
Lipase – 572U/L
Albumin – 3.5g/L
What are the potential causes of this patient’s condition?
This patient has pancreatitis and a helpful mneumonic to remember the most common causes is:
I GET SMASHED

What are 2 scoring systems used to predict severity?
There are 2 common scoring systems to predict or evaluate the severity of pancreatitis. The first is the well known Ranson Criteria, that was introduced in 1974. It uses 2 separate time frames to predict severity. The first is at the time of admission and uses 5 variables:
- Glucose > 200 mg/dL
- AST > 250 U/L
- LDH > 350 U/L
- Age > 55
- WBC > 16,000
If < 3 variables present, then it is considered mild. If ≥ 3 variables present, then it is considered severe.
After 48 hours, a second set of criteria can be used to assess mortality. These variables are:
- Hematocrit decrease of ≥ 10%
- Blood urea nitrogen increase ≥ 5 mg/dL despite fluids
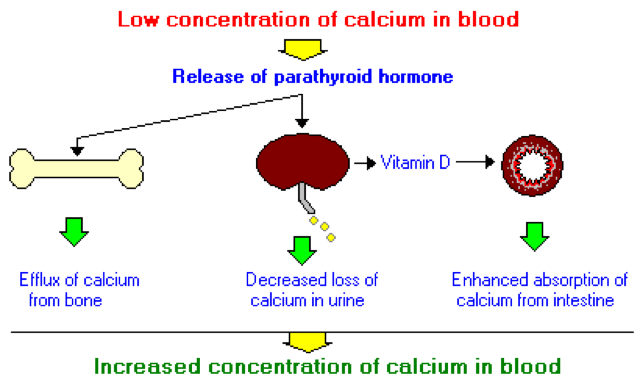
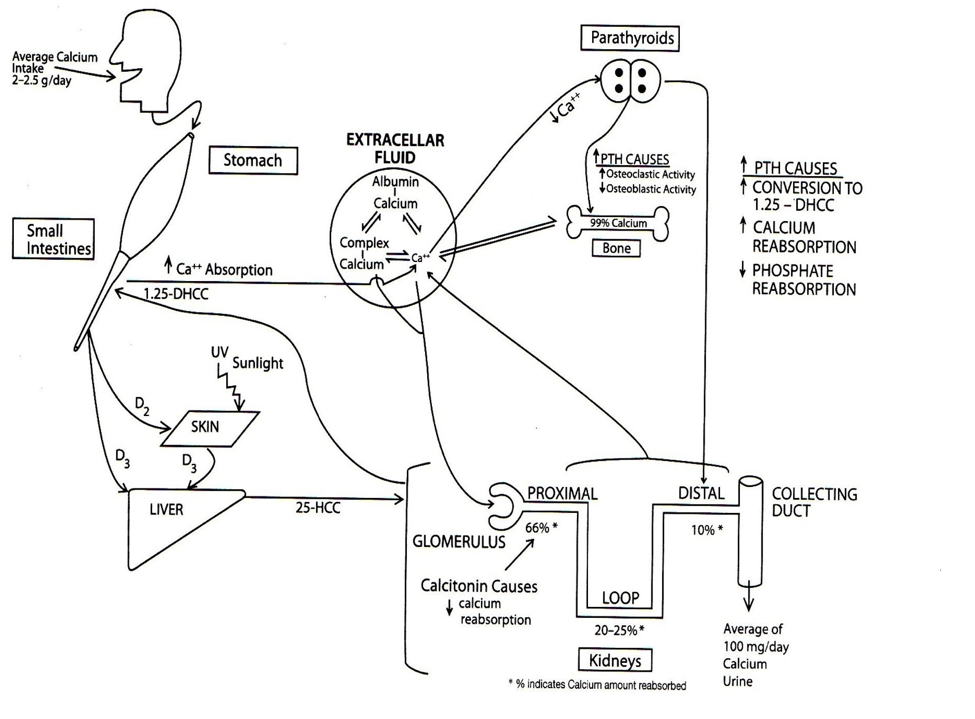
- Serum calcium < 8 mg/dL
- PaO2 < 60 mmHg
- Base deficit > 4 MEq/L
- Fluid resuscitation > 6L
Mortality associated with this is as follows:
- 0-2 – 2%
- 3-4 – 15%
- 5-6 – 40%
- > 6 – 100%
Another scoring system is the modified glascow score for acute pancreatitis. This was first developed in 1984 and modified in 1988. It looks at 8 specific variables to predict severity of acute pancreatitis. The variabls can easily be remembered by the acronym PANCREAS:
- PaO2 < 60 mmHg
- Age > 55
- Neutrophils (WBC > 15,000)
- Calcium < 8 mg/dL
- Renal (BUN > 6 mg/dL)
- Enzymes (LDH > 600 U/L or AST/ALT > 200 U/L)
- Albumin < 3.2 g/L
- Sugar (Glucose > 180 mg/dL)
If < 3 variables, then mild pancreatitis. If ≥ 3 variables, then severe pancreatitis.
Case Conclusion
Our patient in this case would be consider severe pancreatitis (for both scoring systems) due to glucose > 200 mg/dL, LDH > 600 U/L, and and BUN > 6 mg/dL
References
- Blackborne LH. Chapter 55: Pancreas. In: Surgical Recall. 6th edition. Lipincott Williams Wilkins. Philedelphia, PA.
-
Banks PA, Freeman ML, . Practice guidelines in acute pancreatitis. The American Journal of Gastroenterology. 2006;101(10):2379-400. [
pubmed]
-
Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surgery, gynecology & obstetrics. 1974;139(1):69-81. [
pubmed]
-
Leese T, Shaw D. Comparison of three Glasgow multifactor prognostic scoring systems in acute pancreatitis. The British Journal of Surgery. 71988;5(5):460-2. [
pubmed]