19yo male is brought into the emergency department by EMS after getting into an altercation and getting knocked unconscious. He unsure of how long he was out, but he came to once EMS arrived. He denies any nausea, vomiting, or vision changes. He is drowsy/lethargic with his eyes closed, but is arousable to voice. He can carry on a conversation, but he needs frequent redirection and he does not know where he is. While talking with him, the nurse starts an IV and he tries to swat her away with his opposite hand.
What is the classic score we use and what is his score?
The Glasgow Coma Scale (GCS) was first devised in 1974 and has been the predominant neurologic scoring system since. It takes into account 3 main variables and each variable has a point score attached to it. The maximum score is 15 and the minimum score is 3 (3T if intubated).
Eye opening
4 points – Spontaneous
3 points – To speech
2 points – To pain
1 point – None
Verbal Response
5 points – Oriented
4 points – Confused conversation
Not sure where they are, or what their name is
3 points – Inappropriate words
They speak real words, but they are not in context
2 points – Incomprehensible sounds
1 point – None
Motor Response
6 points – Obeys commands
5 points – Localizes to pain
Crosses midline/clavicles to remove painful stimuli
The GCS was never designed to be used for acute injury. It was created to monitor changes in neurologic status of patients in a neurosurgical unit and was not designed to have the 3 individual variables combined into one score. Here are the important limitations of the GCS.
The GCS is NOT reliable
It is made up of subjective elements that are open to the interpretation of each provider assessing the patient and has been repeated shown to have poor inter-rater reliability.
One study showed only a 38% accuracy between raters and were 2 or more points off 33% of the time.
Providers CAN’T remember the scale
It has too many elements and is regarded as too complicated to be easily, and rapidly applied to patients
In 2003, it was discovered that 25% of British hospitals were using the original 12-point scale instead of the current 13-point scale without anyone noticing.
The GCS is only GROSSLY predictive
It is not designed to predict outcomes of patients with acute neurologic injury.
The GCS is NOT equal to the sum of its parts
The original creators vehemently opposed the summed total score because it assumes that each variable is equal to the others in terms of importance
Example
GCS of 4 with 1E + 1V + 2M = 48% mortality
GCS of 4 with 1E + 2V + 1M = 27% mortality
GCS of 4 with 2E + 1V + 1M = 19% mortality
Are there any other scoring systems out there?
The motor subscale of the GCS has been proven to be most predictive of outcomes in patients with neurologic trauma and injury. This has led to debate about whether to do away with the other 2 subscales and use just the motor score (since it has been shown to close to linear in regards to survival).
Healy C. J Trauma. 2003.
But this is still 6 points and some argue can be further simplified. One study broke down the 6-point motor subscale and found that only 3 of those were statistically important. Those are:
Obeys commands
Localizes to pain
Withdrawal to pain or less
This new Simplified Motor Scale can be remembered by the acronym TROLL (Test Responsiveness: Obeys, Localizes, Less). 2 other simplified scores have also been created to help quickly determine neurologic status. These are:
AVPU
Alert
Responds to verbal stimuli
Responds to painful stimuli
Unresponsive
ACDU
Alert
Confused
Drowsy
Unresponsive
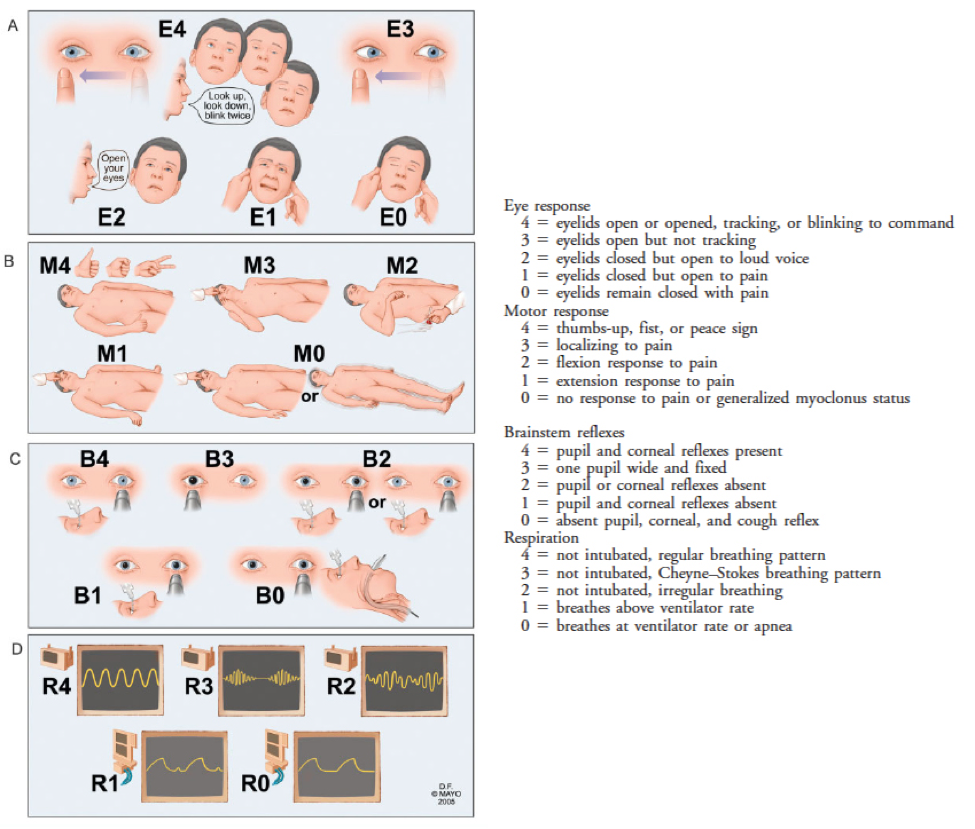
There is another, although more complicated, score called the FOUR score, which has 4 components and stands for Full Outline of UnResponsiveness. Unfortunately, it is even more complicated than the GCS (in the original study it was performed by neurologic specialists, not general practitioners) and it performed just as poorly in external validation studies as the GCS.
Wijdicks EF. Ann Neurol. 2005.
Bottom Line
GCS is essentially worthless clinically even when it is calculated correctly. Simplified scores give just as much information, are easier to use, and are just as predictive. But….you will always be asked “what is the patient’s GCS”, in spite of the growing evidence against it.
19yo male is brought into the emergency department by EMS after getting into an altercation and getting knocked unconscious. He unsure of how long he was out, but he came to once EMS arrived. He denies any nausea, vomiting, or vision changes. He is drowsy/lethargic with his eyes closed, but is arousable to voice. He can carry on a conversation, but he needs frequent redirection and he does not know where he is. While talking with him, the nurse starts an IV and he tries to swat her away with his opposite hand.
What is the classic score we use and what is his score?
“A person who feels appreciated will always do more than what is expected.” (Author unknown)
This quote I came across many moons ago has been ringing in my head for the past few days. Even though I am still considered a “young” professional at 36 and I was born in the transition years between Generation X and Millennials, I still feel I have an old-school professional ethos.
Do your job…work hard…do what is asked…don’t ask for anything….let your work speak for itself.
I know this blog is meant to be educational and to teach you something about medicine so you can better take care of patients in the clinical setting. But…one of the more selfish reason I created it was because I wanted to see the fruits of my labor and feel like I accomplished something important. Academic publishing has always been a fickle beast. You spend weeks to months writing a manuscript and submit it to a journal, only to be judged by a select few that will decide the fate of your work. Sometimes it is accepted….sometimes it is rejected…and sometimes it hangs out in limbo accepted but not published for years (I have 2 papers that I wrote in 2014 that have yet to be published). This is why I started the blog and podcast. I have control over what I do and when it gets out for people to read and listen to.
I think it more important to disseminate information and teach to whoever wants to learn, than to write for journals (that nobody reads) just because “this is what we do in academia”. My hope is this paradigm will shift in the future as more and more people see the benefit non-traditional educational activities and how it can be used as scholarly work. But unfortunately….this is not the day.
I never fancied myself as a writer, but I am starting to have that cathartic feeling that so many writers have. For the 5 or 6 of you that read this blog, thank you. The PAINE Podcast and Blog is the single most important professional endeavor I have ever done because it benefits only you, me, and patients. No journals…no professional societies…no third parties. The feedback I get from my students, the social media universe, and other professionals I work with tells me what I am doing means something and for that, I will always be grateful. To me, that is more important than publications, grant funding, or research.
I leave you with “The Man in The Arena” by Theodore Roosevelt that really sums up how I have been feeling of late.
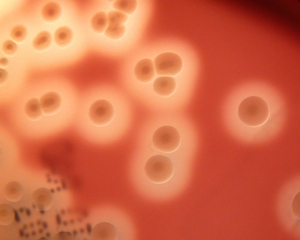
American Academy of Pediatrics. Group A Streptococcal Infections. In: Red Book: 2015 Report of the Committee on Infectious Diseases, 30th, Kimberlin DW, Brady MT, Jackson MA, Long SS (Eds), American Academy of Pediatrics, Elk Grove Village, IL 2015. p.732.
With finals week closely approaching, this weekend snuck up on me quick and I was not able to get a good case together for the blog….my bad.
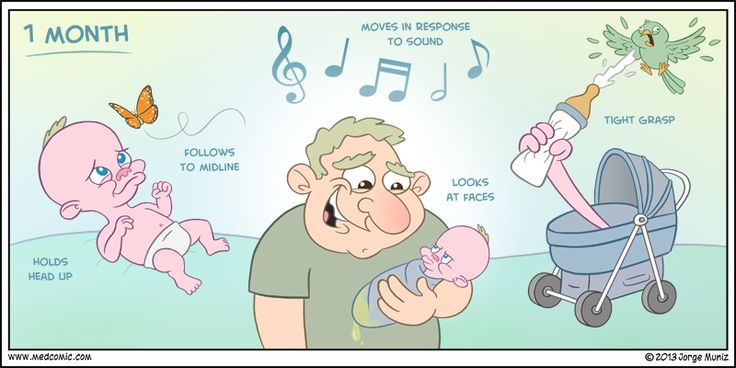
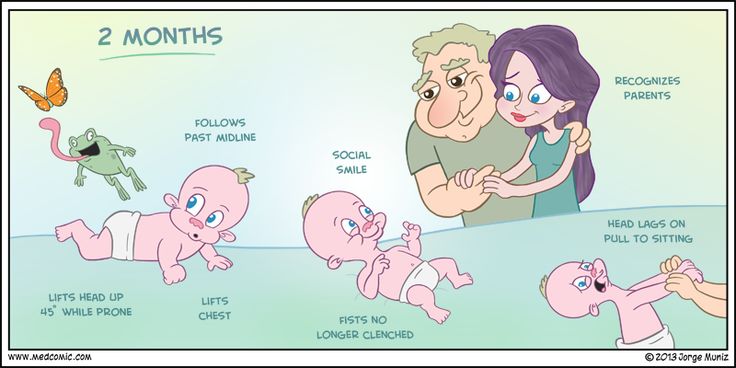
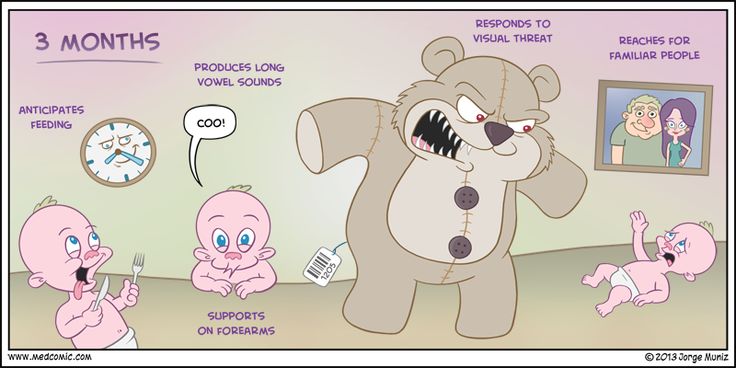
But, FEAR NOT!!!! What I thought I would do for the last post of pediatric month is review the pediatric developmental milestones by way of infographics.
If you haven’t already, you need to be following Jorge Muniz of Medcomic on Twitter and buy his book….it is awesome and he is a fellow PA. I try to incorporate as many of his images as possible when I teach.
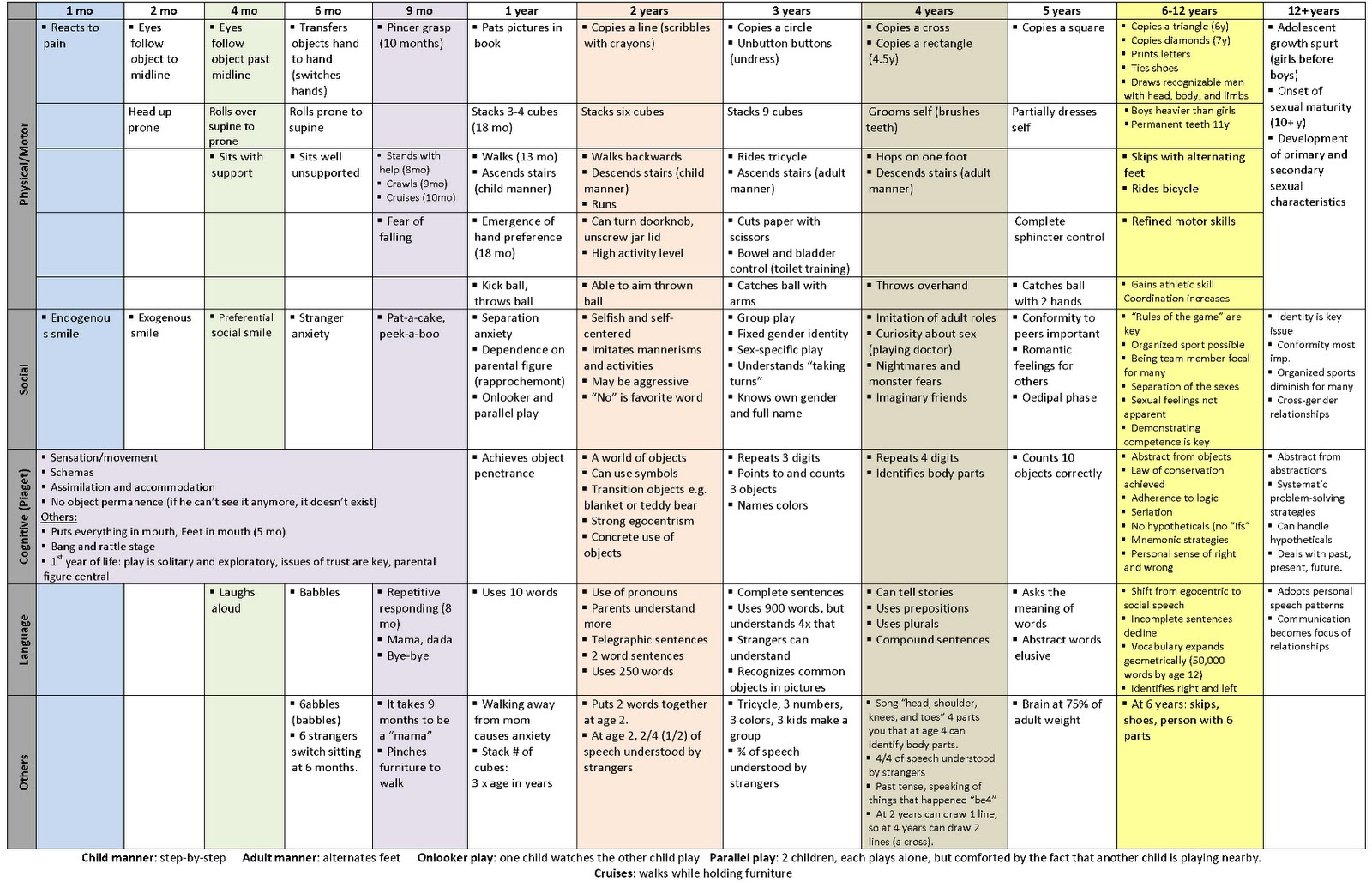
The last graphic is the THE BEST single graphic of developmental milestones (from 1 month to 12 years) I have ever found. Great resource for your pediatric rotation.
Comprise 15% of all CHD and 33% of potentially fatal CHD
Physiology
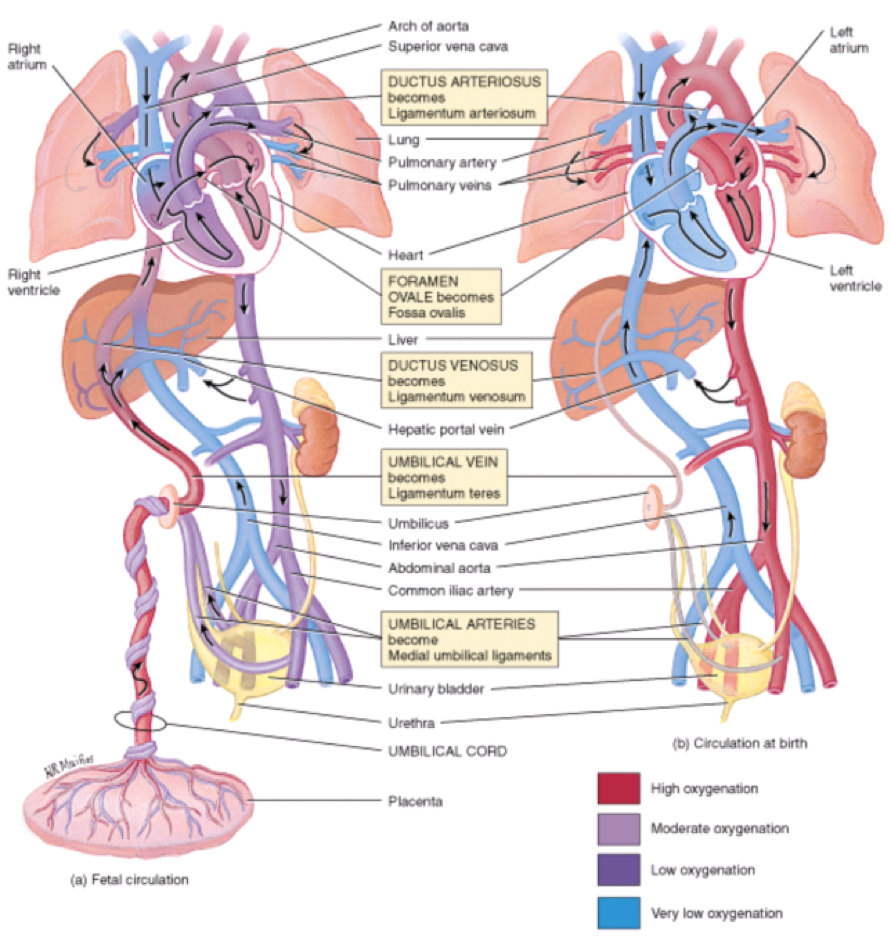
The cardiovascular system in-utero is a complicated machine that is designed to bypass the lungs and provide oxygenated blood from the placenta. There are two main structures that help maintain oxygenation when the fetus’ lungs are not used:
Ductus arteriosus
Connects the pulmonary artery to the descending aorta
Prostaglandin E1 and E2 are produced by the placenta and keep this open
Absolutely vital to remain patent in several of the cyanotic diseases to provide oxygenated blood
Foramen ovale
Communication between right and left atrium
Once the infant begins spontaneously breathing, increases in pulmonary blood flow and left atrial pressures mechanically seals the foramen ovale
Fetal circulation (a) in-utero and (b) during 1st 7 days of life
Khan Academy Tutorials
Cardiac Causes of Cyanosis
3 Main Physiologic Categories
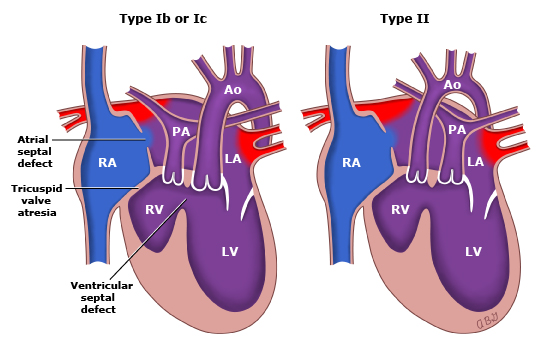
Decreased pulmonary blood flow
Tetralogy of Fallot, tricuspid atresia
Increased pulmonary blood flow
Transposition of great vessels, truncus arteriosis, total anomalous pulmonary venous connection
Severe heart failure
Hypoplastic left heart, coarctation of the aorta
Timing of Presentation
Within 48 hours of birth
Transposition of great vessels, tricuspid atresia
With 7 days of birth
Truncus arteriosus, total anomalous pulmonary venous connection, Tetralogy of Fallot
Screening
Hyperoxia Test
100% oxygen via hood for 10 minutes
Radial artery (preductal) PaO2 is measured
PaO2 > 150 mmHg suggests pulmonary disease
Pulse Oximetry Screening
Measuring the difference in SpO2 between preductal (right hand) and postductal (either foot) flow
A positive test warranting further investigation includes any of the following:
SpO2 < 90% in either extremity
SpO2 90-94% in both locations on three measurements one hour apart
SpO2 difference > 3% on three measurements one hour apart
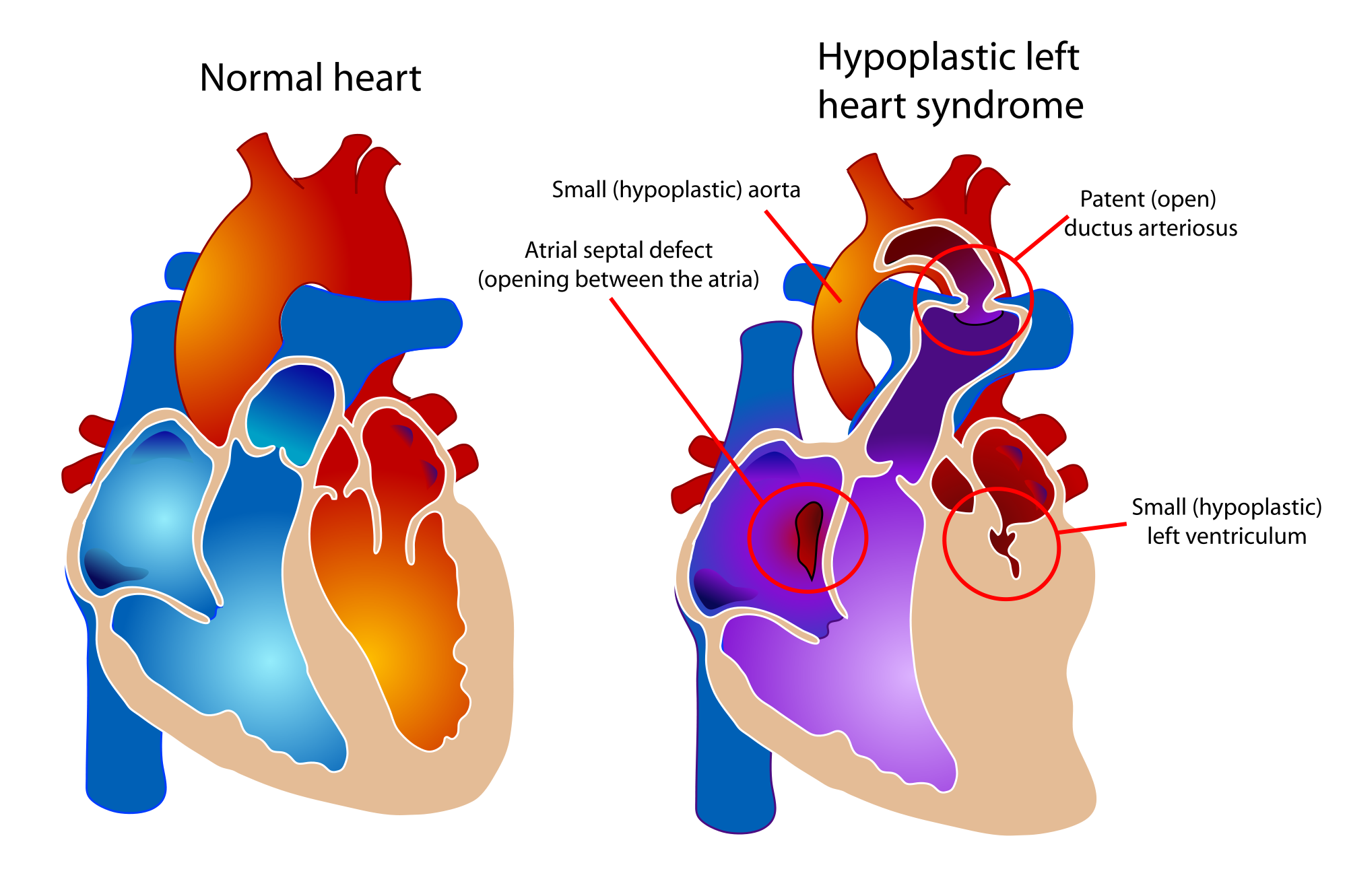
Spectrum of cardiac malformations characterized by underdevelopment of the left ventricle with atresia, stenosis, or hypoplasia of aortic and/or mitral valve, and hypoplasia of ascending aorta and arch
Survival is dependent on PDA and ASD
Signs and Symptoms
Prenatal
Can be diagnosed by fetal ultrasound between 18-24 weeks
Postnatal
“Honeymoon” period while PDA is open and ASD is unrestricted
May be discharged and present after 3-5 days
If ASD is restricted –> rapid decompensation as PDA closes
Single S2 heart sound
No murmur
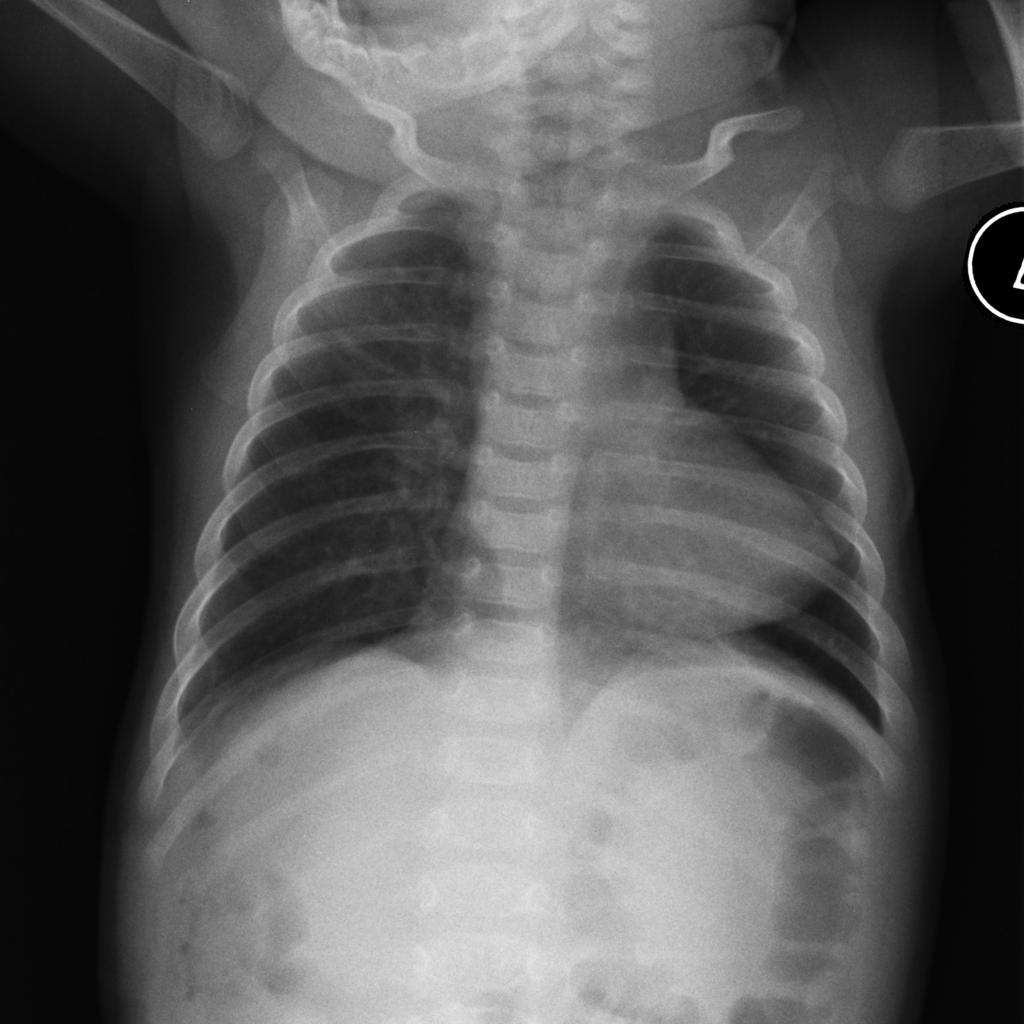
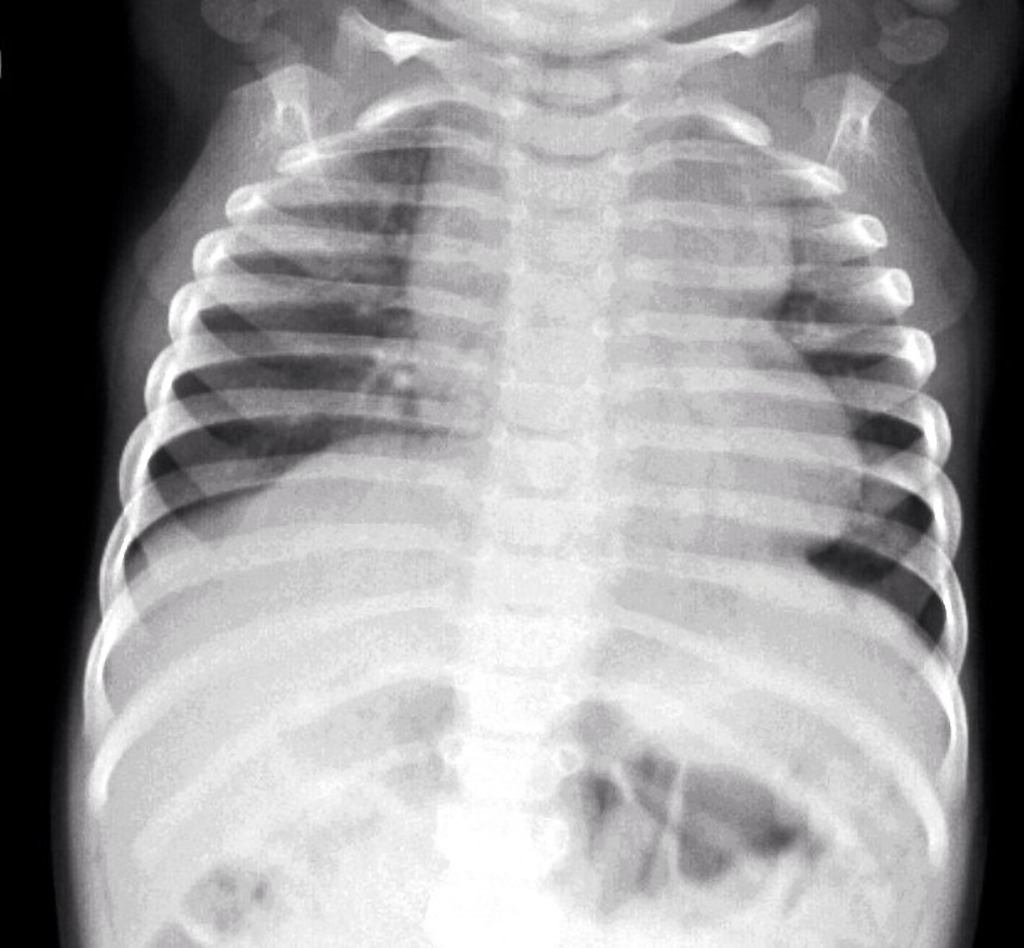
Chest radiograph may show small cardiac silhouette
Electrocardiogram shows RAD, RAE, RVH
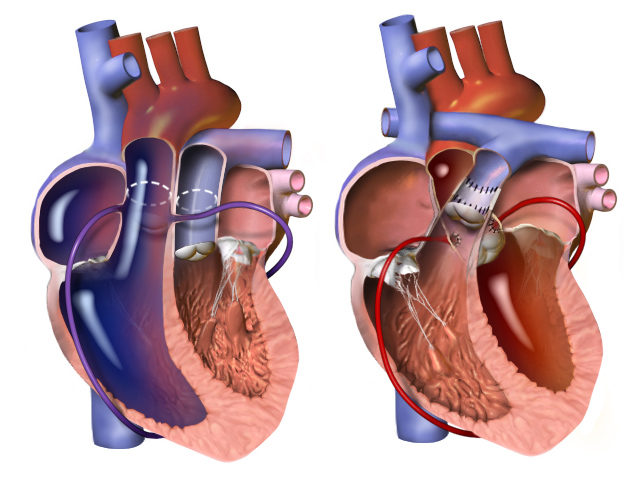
Surgical repair performed in 3 stages
1st stage performed immediately
Norwood procedure (3 parts)
Creation of neoaorta
Blalock-Taussig shunt
Resection of atrial septum
Norwood Procedure
2nd stage performed at 3-6 months
Bidirectional Glenn procedure
Bidirectional Glenn Procedure
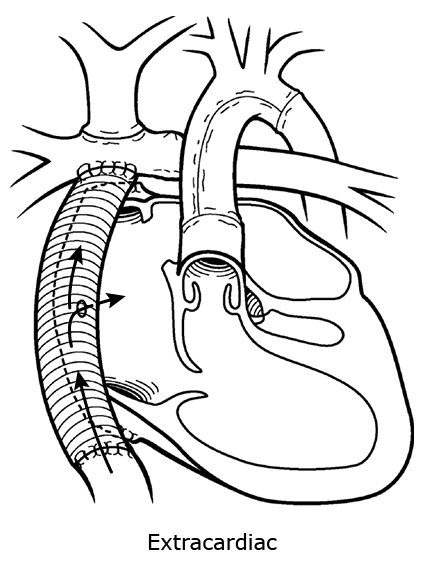
3rd stage performed at 2-3 years
Fontan procedure
Hybrid approach and heart transplant are emerging treatment options
PAINE Pearls to Remember
6 “Ts” of Congenital Cyanotic Heart Defects
Tetralogy of Fallot
Transposition of Great Vessels
Tricuspid Atresia
Truncus Arteriosus
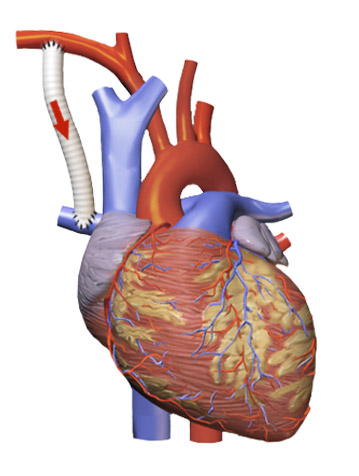
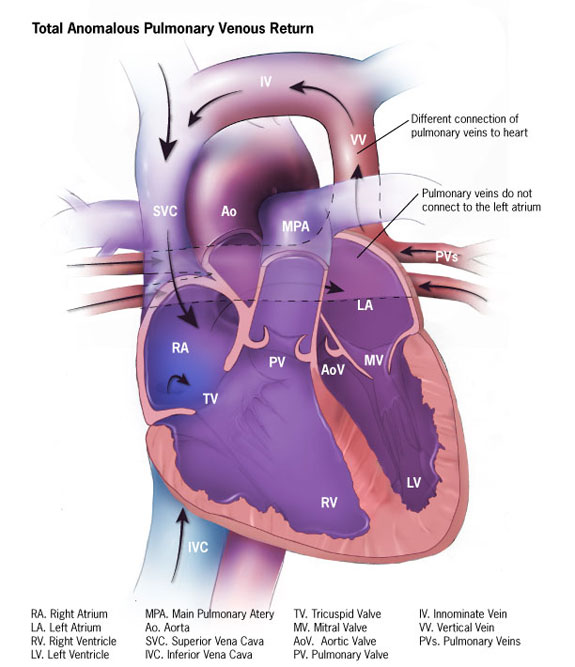
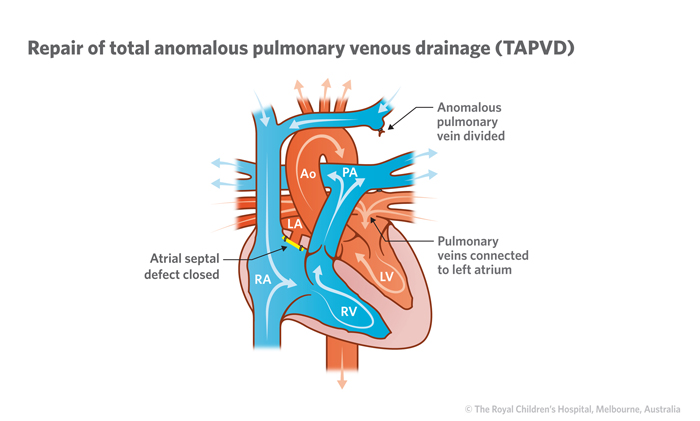
Total Anomalous Pulmonary Venous Connection
“Tiny” (Hypoplastic) Left Heart Syndrome
Numbers of Congenital Cyanotic Heart Defects
1 trunk (truncus arteriosus)
2 great vessels (transposition)
3 “tri” (tricuspid atresia)
4 “tetra” (Tetralogy of Fallot)
5 words (Total Anomalous Pulmonary Venous Connection)
VI – the left “I” is half as big as the right “V” (hypoplastic left heart)
Cottage Physician Reference
Nothing directly related to congenital heart defects, but I did find this quote interesting. It says:
“ The general rule as to tying the cord , with the exceptions above noticed, is, that it is the safest to delay the tying of it, until it has entirely ceased to pulsate”
The OB realm is still debating delayed cord clamping…It looks like everything in medicine always comes full circle





































{kind=link}