What vitamins have a higher potential for causing toxicity and why?
Answer
Fat soluble vitamins can be stored in the adipose tissue instead of excreted if in excess. As a result, vitamins A, D, E, and K can cause toxicity if patients take too much (in this order of incidence as well).
Hypervitamintosis A can result in ataxia, hepatotoxicity, visual impairments, and orange skin.
Hypervitamintosis D can result in hyperphosphatemia and hypercalcemia.
Hypervitamintosis E can block vitamin K absorption and leads to easy bleeding and bruising
Hypervitamintosis K is very rare and really only seen in infants receiving newborn injections after birth.
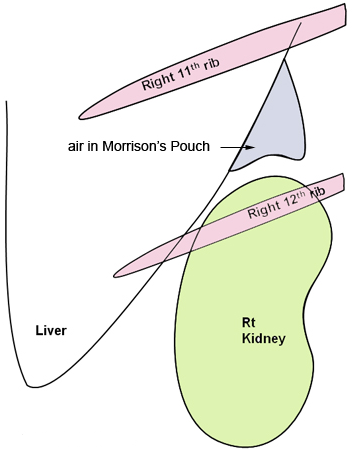
Other known aliases – hepatorenal recess/fossa, right posterior subhepatic space
Definition – a potential space between the liver and the right kidney
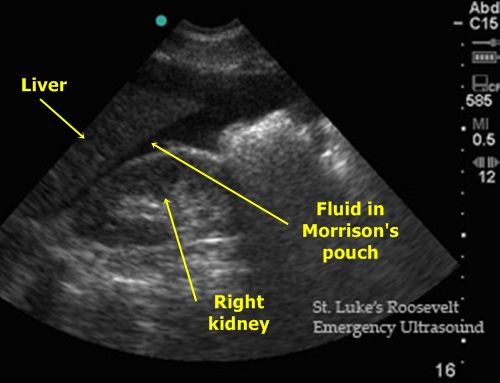
Clinical Significance – This a space where fluid can accumulate in the setting of ascites or abdominal trauma and be seen on CT or ultrasound. It is one of the view of a Focused Assessment of Sonography in Trauma (FAST) exam. Typically, 30-40mL of fluid needs to be present to be visualized.
Ultrasound
Computed Tomography
History – Named after James Rutherford Morison (1853-1939), a British surgeon who received his medical degree from the University of Edinburgh in 1874. He was also an assistant and “surgical dresser” for Joseph Lister early in his career and later founded a school of surgery at the University of Durham where he made his name as a prolific instructor of surgery. He is well known as a pioneer of modern surgery with several of his contemporaries noting he was twenty years ahead of his time and was a driving force of he surgical arts in Great Britain at the turn of the 20th century.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Definition – sac-like outpouching of the mucosa and submucosa through Killian’s triangle, which is the area of structural weakness between the cricopharyngeus and lower inferior constrictor muscles.
Clinical Significance – There are actually three different types of diverticulae that can form in this region and are based on anatomic location:
Zenker’s – immediately above the upper esophageal sphincter
Traction – near midpoint of the esophagus
Epiphrenic – immediately above the lower esophageal sphincter
Signs and symptoms of a Zenker’s diverticulum are pretty awful and include dysphagia, pulmonary aspiration, and halitosis from partially rotting food in the outpoaching. It is diagnosed via barium swallow under flouroscopy. The majority of the patients are male and present after the age of 60. Management is surgical resection.
History – Named after Friedrich Albert von Zenker (1825-1898), who was German physician and pathologist and received his medical doctorate at Leipzig in 1851. He held numerous teaching posts including chief prosector and professor of general pathology and anatomy at Dresden city hospital. Dr. Zenker, along with Hugo Wilhelm von Ziemssen, published a case series and literature review on his eponymous diverticulum in 1867 entitled “Krankheiten des Oesophagus”. He also was the first to document and describe trichinosis in a girl who died in 1860, proving that the once thought harmless parasite could cause severe disease.
Friedrich Albert von Zenker
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
F. A. Zenker and Hugo Wilhelm von Ziemssen: Krankheiten des Oesophagus. Leipzig, 1867
Ueber die Trichinenkrankheit des Menschen. Virchows Archiv für pathologische Anatomie und Physiologie und für klinische Medizin, Berlin, 1860, 18: 561-572.
58yo
male, with DMI controlled with insulin, has blood glucose measurements
in the morning of 205-272 mg/dL for the past week. He reports that his
evening blood glucose measurements before bed range from 103-127 mg/dL.
What are two potential causes of these findings?
Answer
There are two potential causes of early morning hyperglycemia in a diabetic patient on insulin.
Dawn Phenomenon
Due to the early morning rise of cortisol, patients can experience an early morning hyperglycemia as a result
Somogyi Phenomenon
(as covered by last week’s Ep-PAINE-nym)
This was theorized to occur as undetectable hypoglycemia while the
patient was asleep and the resultant hyperglycemia from instrinsic
protective mechanisms.
Other Known Aliases – posthypoglycemic hyperglycemia
Definition – rebounding hyperglycemia in the setting of a undetected hypoglycemic event
Clinical Significance – It had been hypothesized that patients who had a hypoglycemic event during sleep would have rebound hyperglycemia due to the protective mechanism of the body to counteract this. This would result in an undetectable change that would cause hyperglycemia in the morning. This hypothesis has been proven wrong by numerous studies, but it is still a favorite among endocrinologists to pimp their students on.
History –Named after Michael Somogyi (1883-1971), who was a Hungarian American biochemist and received his doctorate degree from the University of Budapest in 1914. He took a position as professor of biochemistry in 1922 at the Washington University’s Medical School in St. Louis, where later that year the first child with diabetes was treated with an insulin prepared by Somogyi himself. His career work revolved around diabetes and theorized that insulin itself could causes unstable diabetes. He published this paper describing the phenomenon that bears his name in 1938 in the Weekly Bulletin of the St. Louis Medical Society entitled “Insulin as a cause of extreme hyperglycemia and instability”. He also went on to develop the test for serum amylase to help diagnose acute pancreatitis. Dr. Somogyi died from a stroke on July 21st, 1971.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
M. Somogyi, “Insulin as a cause of extreme hyperglycemia and instability,” Weekly Bulletin of the St Louis Medical Society, 1938,
Tordjman KM, Havlin CE, Levandoski LA, White NH, Santiago JV, Cryer PE. Failure of nocturnal hypoglycemia to cause fasting hyperglycemia in patients with insulin-dependent diabetes mellitus. The New England journal of medicine. 1987; 317(25):1552-9. [pubmed]
Hirsch IB, Smith LJ, Havlin CE, Shah SD, Clutter WE, Cryer PE. Failure of nocturnal hypoglycemia to cause daytime hyperglycemia in patients with IDDM. Diabetes care. 1990; 13(2):133-42. [pubmed]
58yo male, with DMI controlled with insulin, has blood glucose measurements in the morning of 205-272 mg/dL for the past week. He reports that his evening blood glucose measurements before bed range from 103-127 mg/dL. What are two potential causes of these findings?
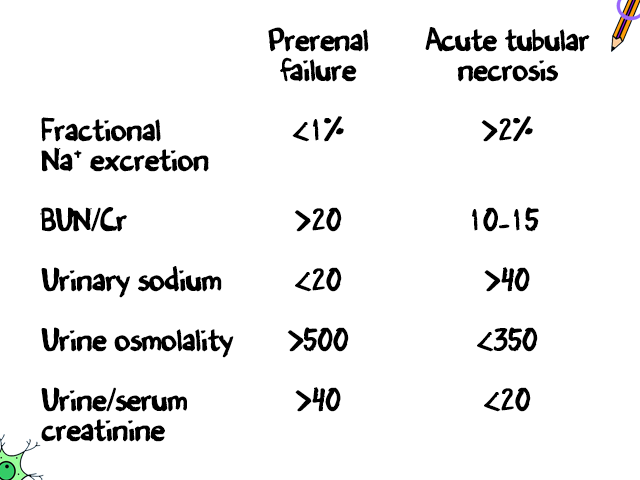
In an oliguric patient, what is the first step in differentiating between prerenal and intrinsic renal causes?
Answer
The fractional excretion of sodium (FENa) can help differentiate prerenal from intrinsic renal causes in patient with oliguria. If the FENa is < 1%, it suggests prerenal and if it is > 2%, it suggests intrinsic renal causes. There are many limitations to using this calculation, but it is a good first step in determining the cause of a patient’s oliguria. Other laboratory studies, such as BUN/Cr, can be useful as well.
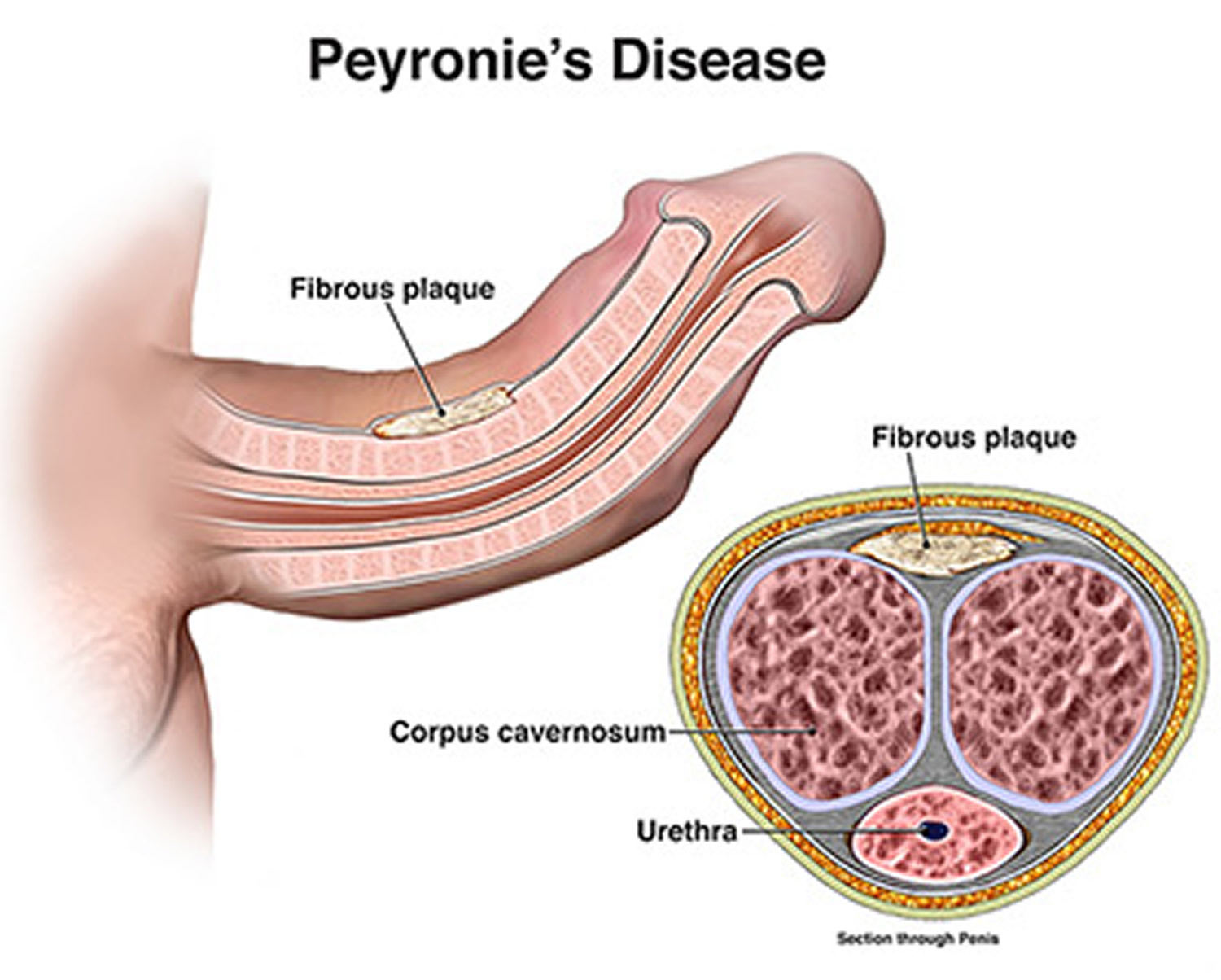
Definition – an acquired, localized fibrotic disorder of the tunica albuginea where thick, fibrous plaques compress the corpora cavernosa
Clinical Significance – The pathogenesis of Peyronie’s disease is unknown and is postulated to be multifactorial. Patients experience pain, penile deformity, and sexual dysfunction
History –Named after François de la Peyronie (1678-1747), who was a French surgeon and received his medical training as a barber-surgeon in Montpellier in 1695. He continued his academic career teaching and practicing surgery and anatomy throughout France. In 1736, he was appointed first-surgeon to King Louis XV and was instrumental in organizing formal training in the surgical arts and was a major force in the creation of the 1743 law that banned barbers from practicing surgery. Also in 1743, he first described the eponymous disease in a book on ejaculation dysfunction where described “indurations of the cavernous bodies like rosary beads” leading to penile curvature. His last name, lapeyronie, means litter stone because his father was a stone cutter. Its a shame he didn’t pursue management of kidney stones as his claim to fame.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.