Question
What are the 5 things to assess in a suspicious lesion/mole to evaluate for melanoma?



What are the 5 things to assess in a suspicious lesion/mole to evaluate for melanoma?

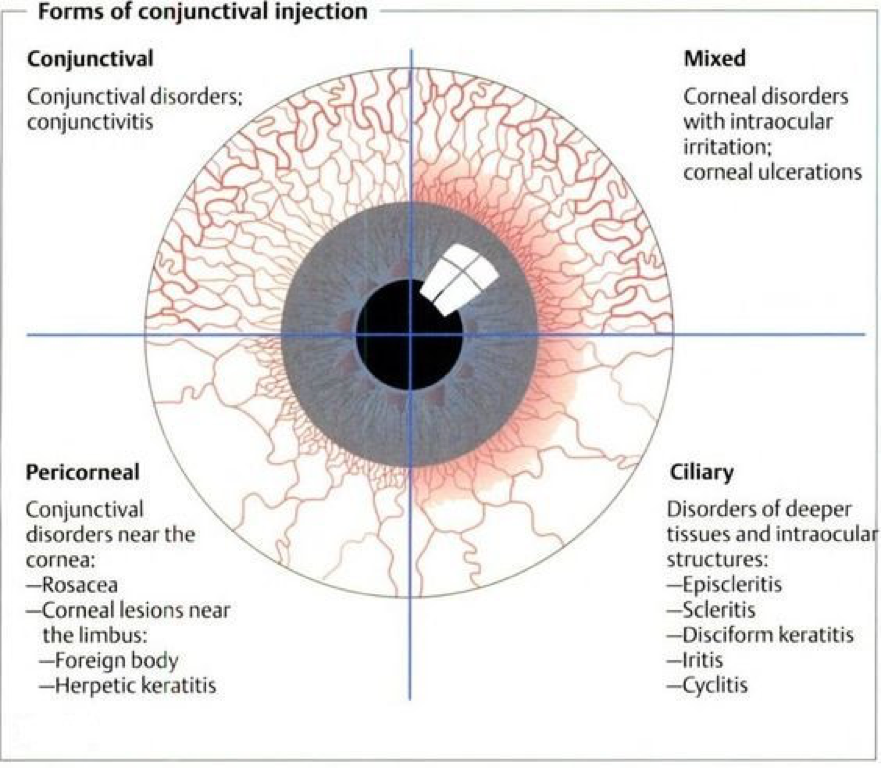
The conjunctiva is a mucous membrane that that lines the surface of the eyelids (palpebral) and globe up to the limbus (bulbar).

The conjunctiva itself is made up of non-keratinized squamous epithelium with goblet cells and substantia propria, which is highly vascularized.

The important thing to remember is that the conjunctiva is transparent, unless inflamed (which is termed “injected”).






These patients are at an increased risk for Pseudomonas infections and should be advised to refrain from wearing their contacts and to have a formal evaluation by an ophthalmologist to rule-out serious infection. Any antibacterial treatment in these patients should also cover for Pseudomonas.
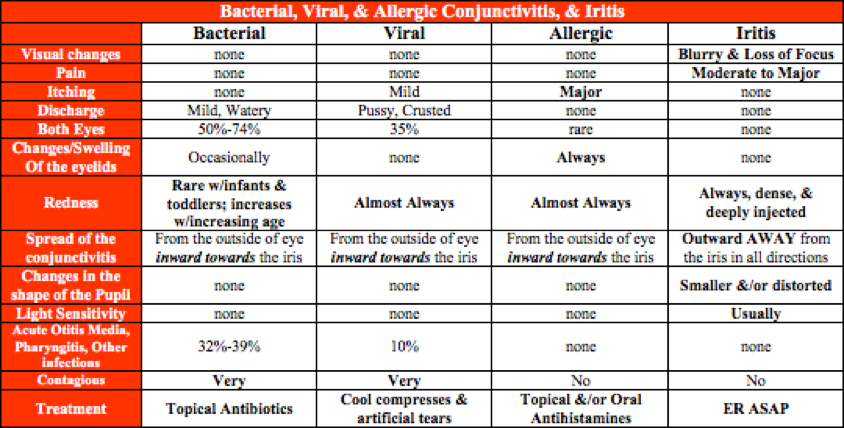
With the exception of gonococcal conjunctivitis, all types are self-limiting and will improve on their own. Having said that, bacterial conjunctivitis will improve faster with topical antibiotics.
Bacterial
Viral and Allergic
Non-Infectious/Non-Allergic
The safest recommendation is to be out until there is no longer any discharge, but this is not practical since it could last for up to 2 weeks.
Viral
Bacterial


Other Known Aliases – Pseudo-isochromatic plates
Definition – Test for detecting color blindness using different color dots to outline numbers
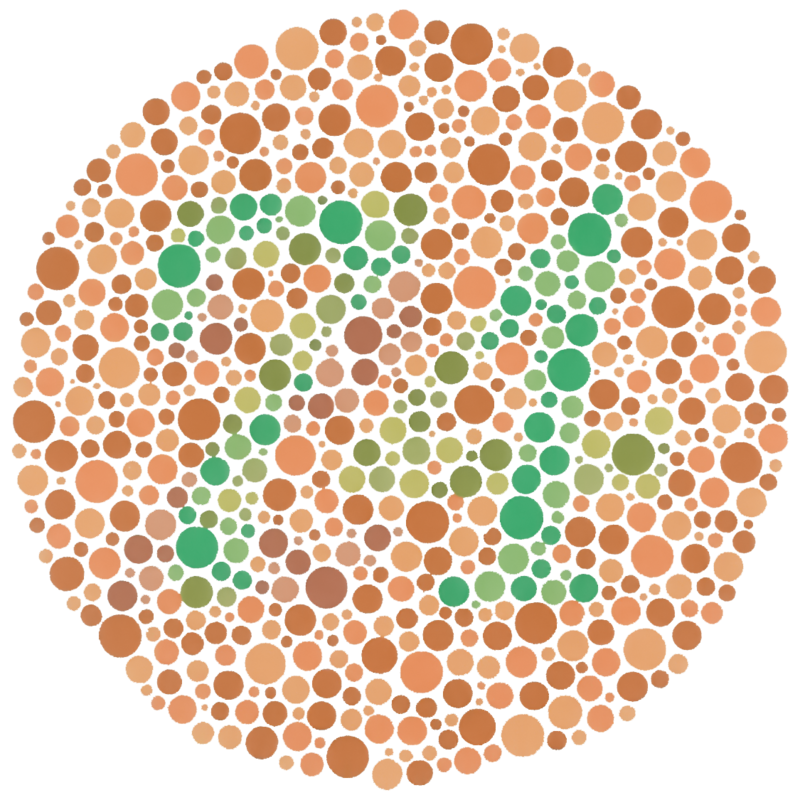
Clinical Significance – Allows for quick assessment of color blindness using different styles plates (a full test is 38 plates) and even differentiate between different types of color blindness. Research has proven that a score of 12 out of 14 red/green plates indicates normal color vision with a sensitivity of 97% and a specificity of 100%.
History – Named after Shinobu Ishihara (1879-1963), who developed these while working as a military surgeon for the Japanese army during World War I as a better way of assessing color blindness in troops. He first published these findings in 1917 in Japan and it was first translated and reviewed in the American Journal of Ophthalmology in June 1918 extolling its usefulness.

References
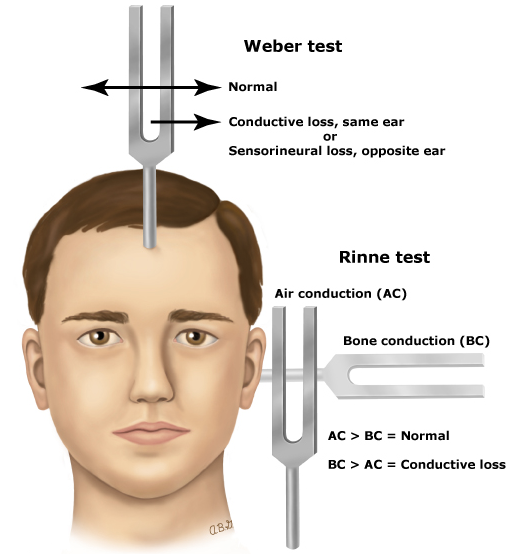
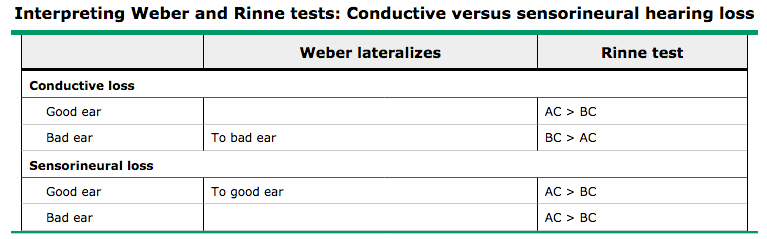
What do you expect to find on Weber and Rinne tests in sensorineural hearing loss (SSNHL)?
Both of these tests are easy bedside maneuvers to perform in the early evaluation of hearing loss and only require a 256 Hz tuning fork. The main thing to remember is that in the Rinne test, air conduction is supposed to be greater than bone conduction….but because the problem with SSNHL is the conversion of sound waves to neural impulses, AC will still be greater than BC because the sound waves can still travel through the canal uninhibited. So AC>BC can be both normal and abnormal, which is why it always done in tandem with the Weber to help figure out which side is affected.
Other Known Aliases – none
Definition – Small, fluid filled cysts on the hard palate of newborns that are most commonly found along the median palatal raphae.

Clinical Significance – None. These are completely normal and occur in 65-80% of newborns. The are formed by epithelium that becomes trapped during palatal development.

History – Named after Alois Epstein (1849-1918), who was a Czechoslovakian pediatrician, graduating from the University of Prague in 1873. His career was highlighted by becoming the first physician-in-chief for the University of Prague hospital in 1873 and being appointed to professor at the University of Prague in 1884. He first described these findings in 1880.


References

Wes Johnson, MSPAS, PA-C, (soon to be), DHSc was a former student of mine at UAB and was a respiratory therapist prior to PA school. He is the Regional Director of Clinical Education for Island Medical Management Emergency group in North Alabama. He won the Preceptor of The Year award from UAB in 2016 and currently finishing up his doctorate degree from A.T. Still University.
Twitter – @wesj2288
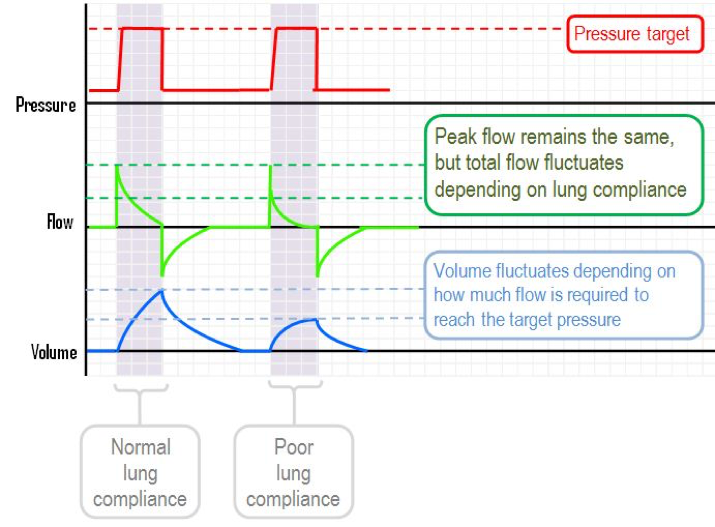
For the purposes of this podcast and post, we will be using the Puritan Bennett 840 ventilator (pictured below). All the term we use are synonymous with all vents, but the screens will be different.

Puritan Bennett 840


(For this section, refer back to the vent picture above)



Mode: AC
Vt: 6-8 mL/kg based on pt’s IBW
Rate: 12-16 bpm
FiO2: 100%
PEEP: 5.0
At the 5-minute mark:
What are some of the chest scores we use to evaluate the likelihood a patient with chest pain is having ACS?

What are the 5 main life-threatening causes of chest pain?

The 5 main life-threatening causes of chest pain you should ALWAYS think of are:

There are a few others that should also cross your mind:
References