For this week’s PAINE PANCE pearl, we will highlight gestational diabetes. Please:
- Describe the two tests
- How they are administered
- How long the tests need
- Laboratory cut-off for diagnosis or further tests


History of FIGO
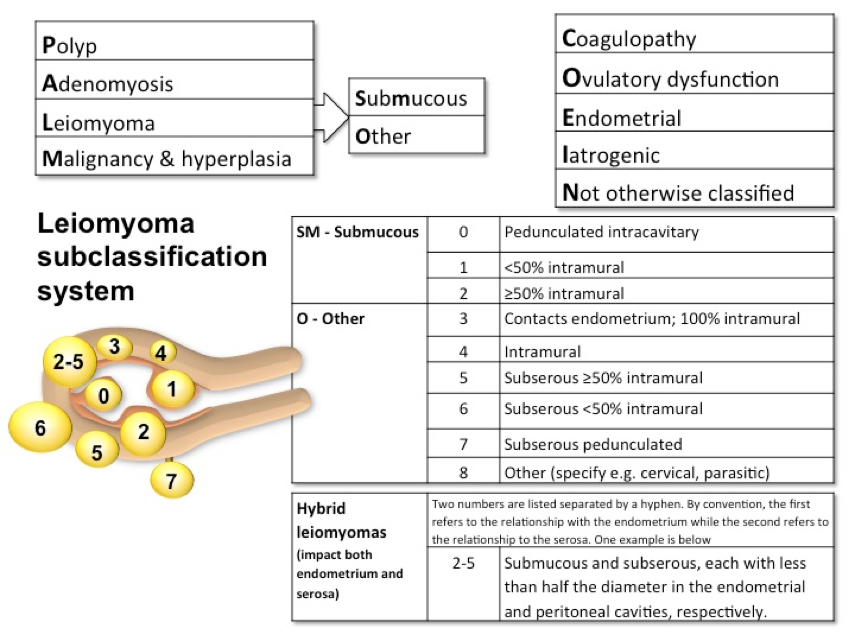
Because of confusing terminology and difficulty in translating to other languages, the International Federation of Obstetrics and Gynecology (FIGO) created a special task force in 2005 charged with clarifying the terminology and classifying the different causes. This way clinicians, patients, and researchers throughout the world could be talking the same language. Dysfunctional uterine bleeding (DUB) was replaced by abnormal uterine bleeding (AUB).. They also introduced a classification system to help sub-divide the causes of AUB.
But in order to define something as “abnormal”, they needed to define normality, which can obviously be very difficult when incorporating the world’s population. The consensus definitions were then agreed upon in 2015 to include the 5th to 95th percentiles form the available data.
The FIGO definition of AUB is any symptomatic variation from normal menstruation, with regards to frequency, regularity, duration, or volume.

Classifications of Abnormal Uterine Bleeding
In 2011, FIGO created a classification system for the main causes of AUB. It is broken down into 2 main categories based on whether or not the pathology can be seen on imaging or histopathology. This also allows for subclassifications due to multiple etiologies.
Documentation
Very similar to the documentation for an OB patient (TPAL score), the documentation uses the PALM-COEIN scoring system for “simplicity”. Example:
References

Definition – Blue discoloration of the cervix and vaginal mucosa seen in early pregnancy.
Clinical Significance – Due to increased blood flow to support a newly implanted embryo and can be seen 6-8 weeks after conception.
History – Given to James R. Chadwick, an American gynecologist of the late 19th century, after he read a paper before the American Gynecologic Society in 1886, but 1st described by Etienne Jacquemin in 1836. Dr. Chadwick did give appropriate recognition to Dr. Jacquemin during this presentation.
References
82-year-old male, with a history of HTN, HLD, and CAD, presents to your clinic with a six-month history of dyspnea on exertion. He states he is unable to walk as far as he used when exercising, and when he over exerts himself, he reports having some mild chest pain and feeling lightheaded. This resolves with rest and he denies any syncope with these events.
Medications
Metoprolol 50mg daily
Lisinopril 10mg daily
Simvastatin 30mg daily
Vital Signs
BP – 158/97
HR – 62
RR – 13
O2% – 100%
Physical exam
General – WN/WD male in NAD
Pulmonary – CTA without adventitial breath sounds
CV – Soft S2 with murmur over right 2nd intercostal space
PV – carotid pulse is weak and has a slow rise, murmur is appreciated
Neuro – No focal deficits
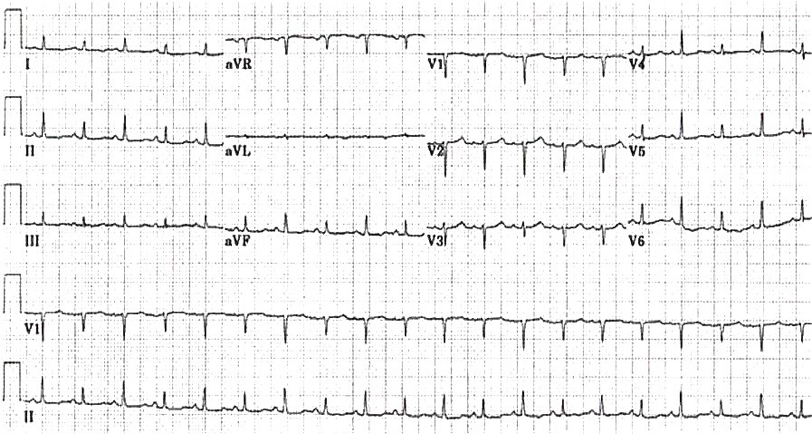
EKG

This patient has aortic stenosis. The suggestive parts of the H&P are:


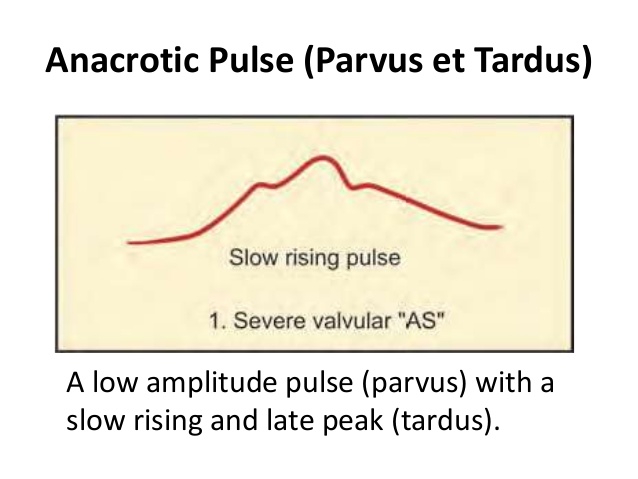
These variables will help with staging the severity of the stenosis, as well as determine need for operative intervention.
Other known aliases – Atrial Reflex
Definition – Compensatory increase in heart rate caused by a rise in right atrial pressure. Opposite of carotid baroreceptors.
Clinical Significance – Respiratory sinus arrythmia. Inspiration causes increased venous return.
History – Described by Francis Arthur Bainbridge in 1915
References

82-year-old male, with a history of HTN, HLD, and CAD, presents to your clinic with a six-month history of dyspnea on exertion. He states he is unable to walk as far as he used when exercising, and when he over exerts himself, he reports having some mild chest pain and feeling lightheaded. This resolves with rest and he denies any syncope with these events.
Medications
Metoprolol 50mg daily
Lisinopril 10mg daily
Simvastatin 30mg daily
Vital Signs
BP – 158/97
HR – 62
RR – 13
O2% – 100%
Physical exam
General – WN/WD male in NAD
Pulmonary – CTA without adventitial breath sounds
CV – Soft S2 with murmur over right 2nd intercostal space
PV – carotid pulse is weak and has a slow rise, murmur is appreciated
Neuro – No focal deficits
EKG
Questions

Anatomy
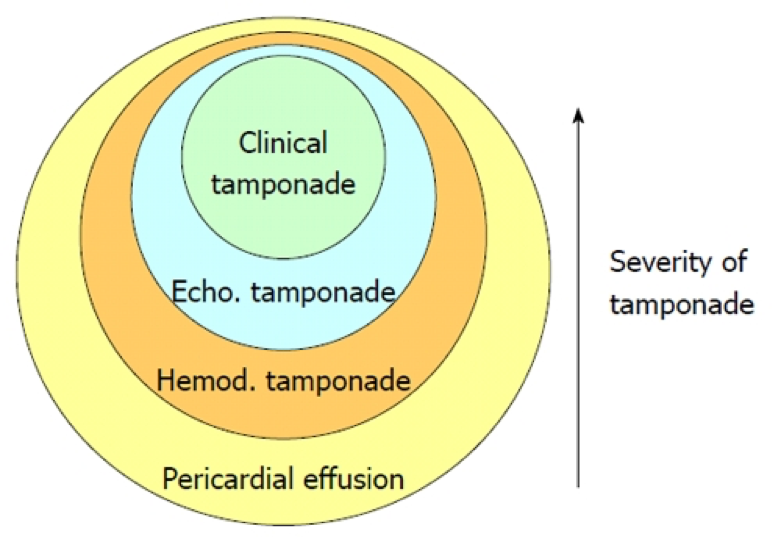
The pericardium consists of a double-layered semi-elastic sac that holds the heart in the mediastinum. Basically, so the heart doesn’t flop around inside the thoracic cavity. There should be a small amount of fluid (15-50mL) present to prevent adhesion of the pericardial sac to the heart. It is then termed an effusion when it is more than the normal amount. How much quantifies an effusion? Doesn’t matter…. what does matter is how fast that fluid develops. Because the pericardium is semi-elastic, it can accommodate and stretch over time if the accumulation is slow. This would lead to a greater volume of fluid before symptoms occur. If the fluid accumulates rapidly, less volume can produce profound effects due to the restrictive nature of the fibrous pericardium.

Etiology
Signs and Symptoms
There are no reliable historical clues or physical exam findings that are specific to pericardial effusions. They are helpful, though, to sort out the cause of the effusion. Common findings include:
Work-Up
Life In The Fastlane – o http://lifeinthefastlane.com/ecg-library/basics/low-qrs-voltage/
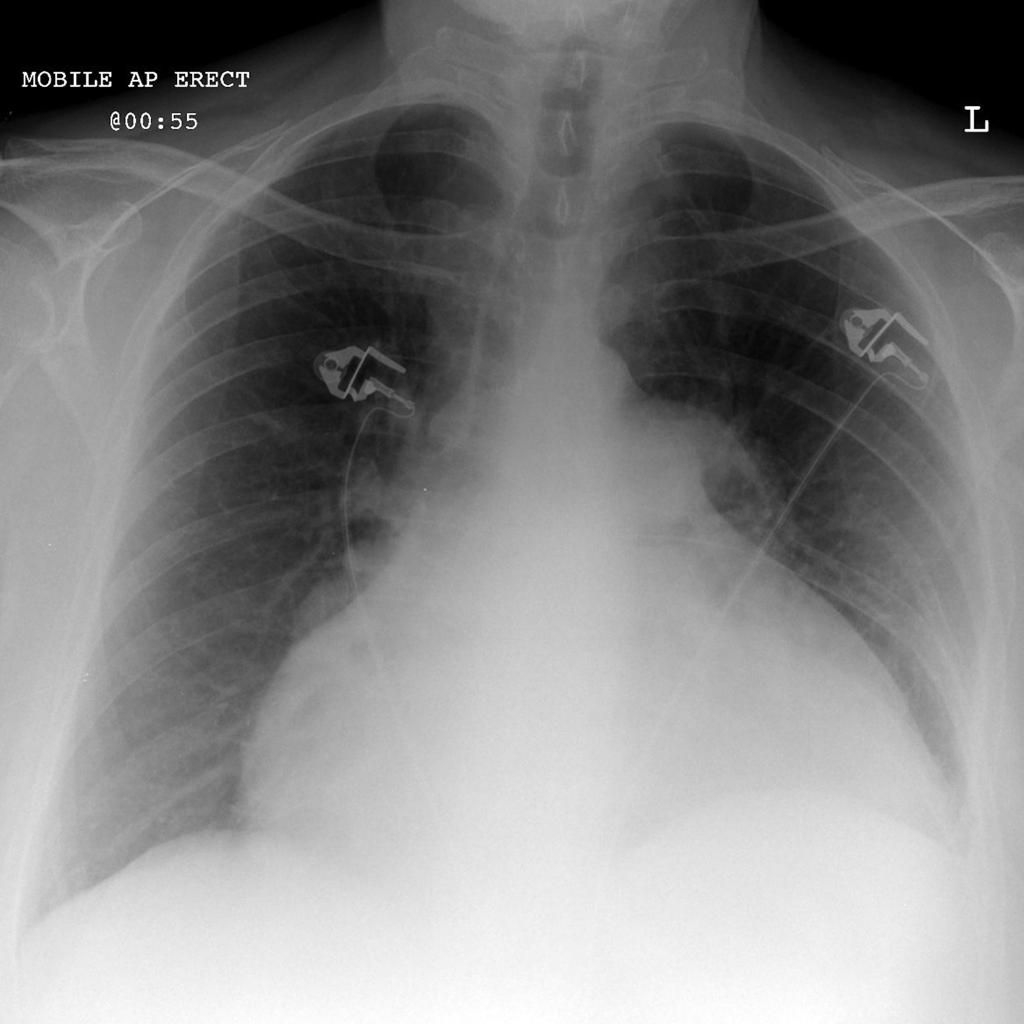
Radiopaedia

Treatment
References
Question
What are the 3 eponymous physical exam findings in patients with bacterial endocarditis and who were they named after?
Answers
Osler Nodes

Janeway Lesions

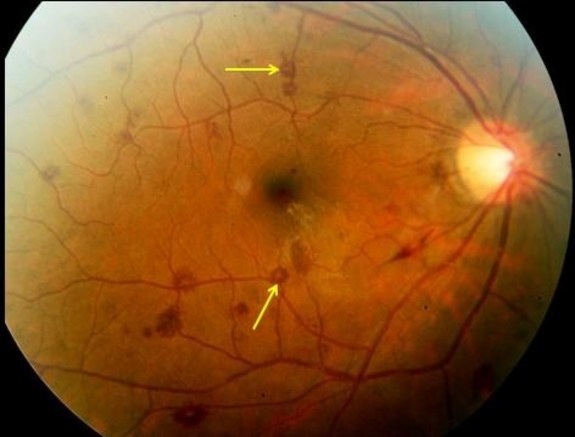
Roth Spots
References
Happy 2017!!! I apologize for the delay in having the pearls coming out, but life is life. So here you go:
What are the 3 eponymous physical exam findings in patients with bacterial endocarditis and who were they named after?

Vector
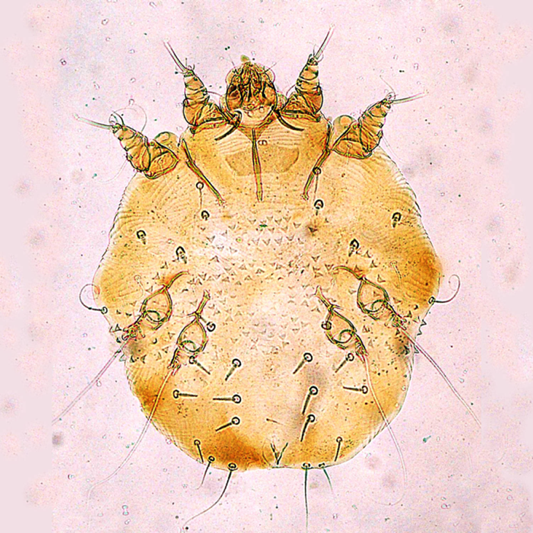
Sarcoptes scabiei
Scabies is caused by the mite Sarcoptes scabiei, which is a whitish-brown, eight-legged mite and it just barely visible by the naked eye at its largest size of 0.4×0.3mm. Only the female mite causes the dermatologic manifestations seen in scabies, as it burrows into the epidermis down to the stratum granulosum layer to lay her eggs.

The female mite can grow these burrows up to 2mm per day and lay 2-3 eggs, up to a total of 10-25 eggs. These eggs hatch after 3-4 days, molt multiple times, and burrow to the surface to mate and then return to continue this viscous cycle. Typically, incubation takes 3-6 weeks after infestations until symptoms present.
Transmission
Scabies are transmitted from direct contact with an infected person and most commonly is sexually acquired. Although not as common, transmission has also been reported to occur through contaminated clothing or bedding as these mites can survive off a host for up to 24-36 hours. Animals can contract scabies, but these rarely cause disease in humans, as they do not reproduce on human hosts.
Risk Factors
Signs and Symptoms
The typically manifestation of scabies is an intensely pruritic rash that is worse at night. The lesions of the rash are small, erythematous, papules typically with an excoriated, hemorrhagic crust. The burrows that may be seen are thin gray/brown/red lines up to 20mm in length.


Areas most common infected are: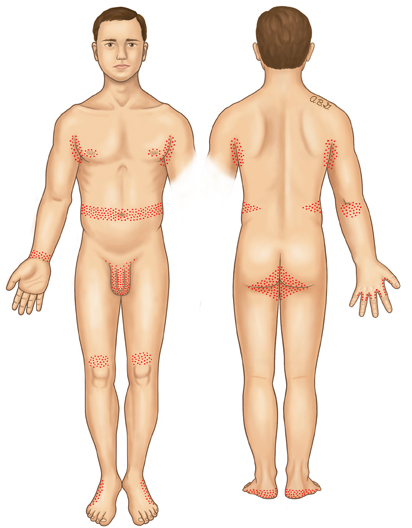
Head, face, and back are not commonly seen and this is theorized to be due to the increased oil production in these areas.
Crusted (Norwegian) Scabies
Immunocomprimised, eldery, debilitated, or disabled patients are at increased risk of developing this severe form of scabies. These mites are not more virulent, but because of their underlying medical conditions, the concentration of mites is much more numerous. These patients develop thick crusts and are highly contagious due to the overwhelming contamination.

Diagnosis
This should be a diagnosis of history and physical exam alone. Skin scrapings can visualize the mites or eggs under the microscope.
Dermoscopy can be used to see the mite in burrow and is classically referred to as the “delta wing” sign, which is the dark head of the mite at the end of a burrow.

“delta wing” sign
Treatment
Prevention of Re-infestation
Recommendations are for all close-contact household members to be treated simultaneously, even if asymptomatic, to prevent cross contamination and re-infestation. Patients should be instructed to wash all clothing/bedding on the hot water cycle with high heat drying to kill any mites. Stuffed animals, jackets, or any other objects not feasible to wash, can be isolated in a plastic bag for 3 days. Fumigation is not necessary
References


