What are the 3 eponymous physical exam findings in patients with bacterial endocarditis and who were they named after?
Answers
Osler Nodes
Painful, erythematous nodules of the hands and feet
Named after Sir William Osler in 1908.
Janeway Lesions
Nontender, erythematous or hemorrhagic macular or nodular lesions on the palms or soles
Named after Theodore Caldwell Janeway in the late 1800s.
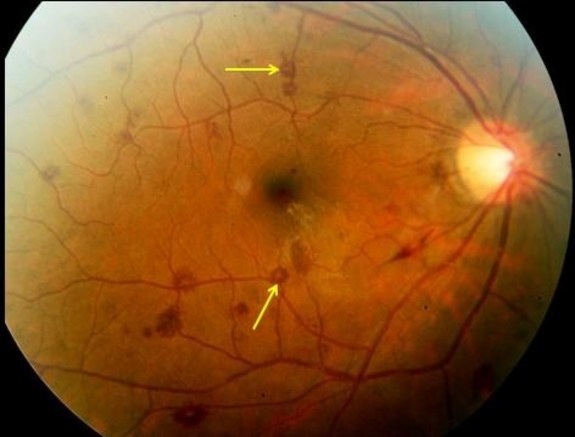
Roth Spots
Retinal hemorrhages with white or pale centers.
Named after Swiss pathologist Mortiz Roth in 1872
References
Osler W. Chronic Infectious Endocarditis. Quarterly Journal of Medicine. 1908;2:219-230.
Ruiz-García J, Canal-Fontcuberta I. Diagnosis of Active Infective Endocarditis from Examination of the Toes and Soles. The American Journal of Cardiology. 2016;118(7):1094. [pubmed]
Khanna N, Roy A, Bahl VK. Janeway lesions: an old sign revisited. Circulation. 2013;127(7):861. [pubmed]
Sethi K, Buckley J, de Wolff J. Splinter haemorrhages, Osler’s nodes, Janeway lesions and Roth spots: the peripheral stigmata of endocarditis. British Journal of Hospital Medicine. 2013;74(9):C139-42. [pubmed]
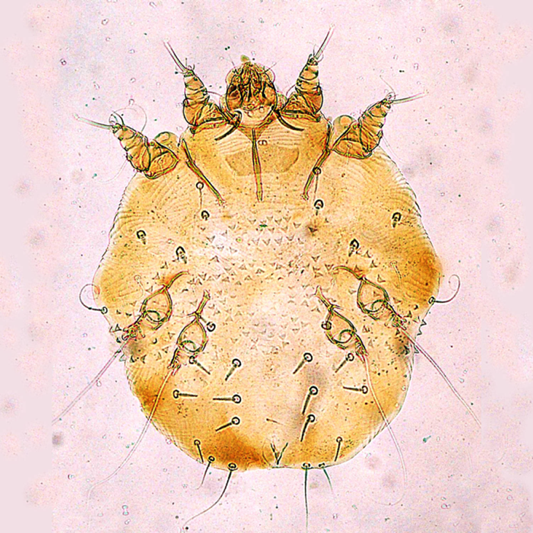
Scabies is caused by the mite Sarcoptes scabiei, which is a whitish-brown, eight-legged mite and it just barely visible by the naked eye at its largest size of 0.4×0.3mm. Only the female mite causes the dermatologic manifestations seen in scabies, as it burrows into the epidermis down to the stratum granulosum layer to lay her eggs.
The female mite can grow these burrows up to 2mm per day and lay 2-3 eggs, up to a total of 10-25 eggs. These eggs hatch after 3-4 days, molt multiple times, and burrow to the surface to mate and then return to continue this viscous cycle. Typically, incubation takes 3-6 weeks after infestations until symptoms present.
Transmission
Scabies are transmitted from direct contact with an infected person and most commonly is sexually acquired. Although not as common, transmission has also been reported to occur through contaminated clothing or bedding as these mites can survive off a host for up to 24-36 hours. Animals can contract scabies, but these rarely cause disease in humans, as they do not reproduce on human hosts.
Risk Factors
Colder temperatures
Higher humidity
Crowded areas with close contact
Signs and Symptoms
The typically manifestation of scabies is an intensely pruritic rash that is worse at night. The lesions of the rash are small, erythematous, papules typically with an excoriated, hemorrhagic crust. The burrows that may be seen are thin gray/brown/red lines up to 20mm in length.
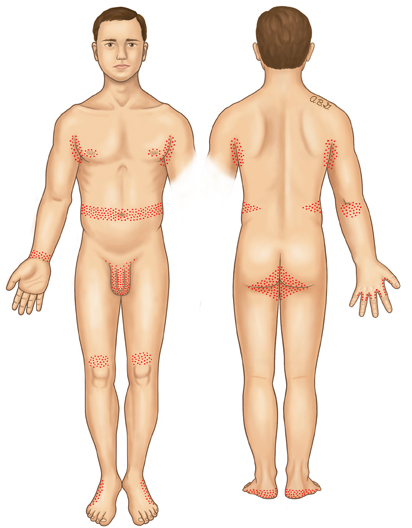
Areas most common infected are:
Webs of fingers
Flexor surface of wrist
Extensor surface of elbow
Axilliary folds
Peri-areolar
Periumbilical
Inguinal folds
Genital regions
Extensor surface of knees
Head, face, and back are not commonly seen and this is theorized to be due to the increased oil production in these areas.
Crusted (Norwegian) Scabies
Immunocomprimised, eldery, debilitated, or disabled patients are at increased risk of developing this severe form of scabies. These mites are not more virulent, but because of their underlying medical conditions, the concentration of mites is much more numerous. These patients develop thick crusts and are highly contagious due to the overwhelming contamination.
Diagnosis
This should be a diagnosis of history and physical exam alone. Skin scrapings can visualize the mites or eggs under the microscope.
Dermoscopy can be used to see the mite in burrow and is classically referred to as the “delta wing” sign, which is the dark head of the mite at the end of a burrow.
“delta wing” sign
Treatment
Topical
Permethrin 5% cream
Apply from jaw line to the soles of feet
Leave overnight (8-14 hours) and washed off the next day
May be repeated 1-2 weeks later
Special populations
Category B in pregnancy
Safe in infants < 1 month
Crusted (Norwegian)
Daily application x 7 days, then 2x/wk until cured
Systemic
Ivermectin (3mg tabs)
2 mg/kg single dose
Single dose not as effective as single application of permethrin
2nd dose, 1 week later as effective as single application of permethrin
Recommended for large outbreaks, multiple infections in a single-household
Not recommended in pregnancy or children < 15kg
Crusted (Norwegian)
2 mg/kg/dose given on day 1, 2, 8, 9, and 15
Pruritus
Hydroxyzine 25mg q6hr
Mirtazapine 4.5-15mg qHS
Prednisone – 2-week taper starting at 60mg/day
Prevention of Re-infestation
Recommendations are for all close-contact household members to be treated simultaneously, even if asymptomatic, to prevent cross contamination and re-infestation. Patients should be instructed to wash all clothing/bedding on the hot water cycle with high heat drying to kill any mites. Stuffed animals, jackets, or any other objects not feasible to wash, can be isolated in a plastic bag for 3 days. Fumigation is not necessary
References
Romani L, Steer AC, Whitfeld MJ, Kaldor JM. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet. Infectious diseases. 2015;15(8):960-7. [pubmed]
Chosidow O. Clinical practices. Scabies. NEJM. 2006;354(16):1718-27. [pubmed]
Heukelbach J, Feldmeier H. Scabies. Lancet. 2006;367(9524):1767-74. [pubmed]
Johnston G, Sladden M. Scabies: diagnosis and treatment. BMJ. 2005;331(7517):619-22. [pubmed]
Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. NEJM. 2010;362(8):717-25. [pubmed]
Fuller LC. Epidemiology of scabies. Current Opinion in Infectious Diseases. 2013;26(2):123-6. [pubmed]
Strong M, Johnstone P. Interventions for treating scabies. The Cochrane database of systematic reviews. 2007. [pubmed]
Romani L, Whitfeld MJ, Koroivueta J. Mass Drug Administration for Scabies Control in a Population with Endemic Disease. NEJM. 2015;373(24):2305-13. [pubmed]
Usha V, Gopalakrishnan Nair TV. A comparative study of oral ivermectin and topical permethrin cream in the treatment of scabies. Journal of the American Academy of Dermatology. 2000;42(2 Pt 1):236-40. [pubmed]
Chambliss ML. Treating asymptomatic bodily contacts of patients with scabies. Archives of Family Medicine. 2000;9(5):473-4. [pubmed]
2.5 years of blood, sweat, tears, late nights, early mornings, angry attendings, sweet patients, amazing staff, and lots and lots of coffee…..but you made it. I am sure it feels like both an eternity and a blink of an eye.
You have made life long friends through this journey and now, you gain 9 faculty members as new colleagues.
As you are standing in the processional line on Friday awaiting your diploma and you are reflecting over your time in PA school, I want you to think back to 2013.
The hardest part of the CASPA application is the personal statement. Think about the self-reflection you did as you struggled to put into words the feelings you had about wanting to become a PA. Think about all your personal, professional, and academic trials and tribulations that led you to the moment that you decided to click on the “Begin a New Application” on the CASPA website. Think about all the medical professionals you encountered, both good and bad, and how you said to yourself “when I am a PA, I will definitely do or not do that”. Remember what that future PA looked like?
That is you now.
My request is simple….be the PA you said you wanted to be in your personal statement 3 years ago.
Don’t let you down.
You certainly have not let me down. There was reason I did not include your class on my “Open Letter to My Students” blog post a few weeks ago. You deserved your own recognition. I am proud of each and everyone of you and I am even prouder to call you all colleagues. You will make great PAs and will make an indelible mark on the world of medicine wherever you practice.
6-year-old boy is brought in my his mother to the office for evaluation of a 3-day history of irritability, fever, and ear pain. She also says that his older sister has had a cold the past week, but it doesn’t seem to be that bad. He is up to date on his immunizations. She also report she has had an intermittent, non-productive cough, but denies any decrease in eating/drinking, diarrhea, or vomiting.
Vital signs show a BP-117/72, HR-94, RR-16, O2-100%, and T-99.2. Physical exam reveals:
General – Non-toxic appearing, NAD, WN/WD
Skin – no rash
Eye – sclera white, conjunctiva clear
Ear – (below)
Throat – OP clear, no erythema or tonsillar swelling
Neck – no LAD
Heart – RRR without M/G/R
Lung – CTA without adventitial sounds
Abdomen – S/NT/ND
PV – 2+ pulses throughout, BCR < 2s
Neuro – No focal deficits
Mother is wanting an antibiotic because the holiday season is here and she can’t afford to have him sick.
What is your diagnosis?
What is your treatment?
What do you tell the mother?
Answer
Diagnosis
Viral Otitis Media
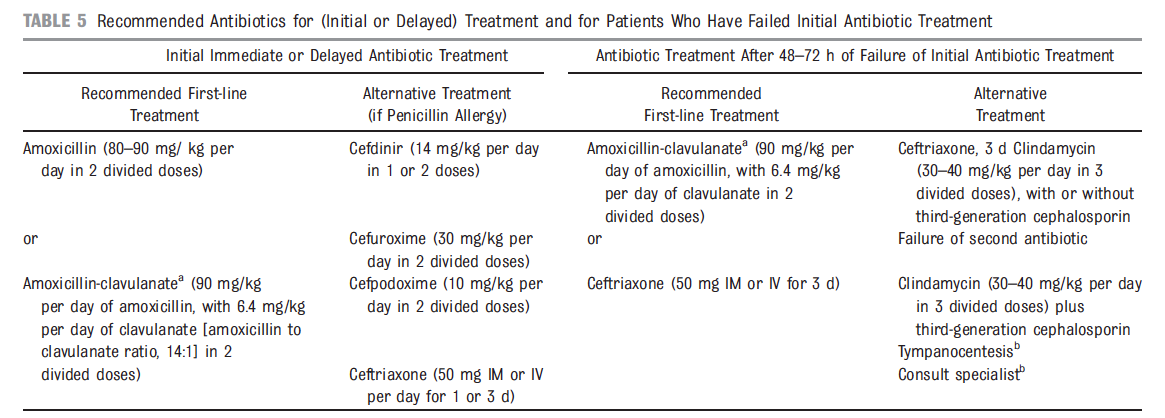
Based on the 2013 consensus guidelines from Pediatrics, the following findings suggests a viral etiology:
Non-toxic appearance
Non-bulging tympanic membrane
> 48hr onset of symptoms
Temperature < 39°C (102.2°F)
No middle ear effusion
Treatment
Given the patient’s age (6yo), there are 2 acceptable options:
Observation
This is the ideal patient for close observation as it is most likely viral, immunocompetant, no ottorhea, no severe symptoms, and non-toxic appearing. Treatment should be directed towards pain control and recommendations should be given to the parents on how to treat:
Ibuprofen – 10mg/kg TID
Acetaminophen – 10mg/kg TID
Topic antipyrine/benzocaine – no longer available
Topical lidocaine – off label, but can be used
Antibiotic Therapy
If the patient fails to improve in 48-72hr, then antibiotics are warranted. Duration of therapy for children > 2yo is 5-7 days.
Case Resolution
After examination of the patient and discussion with the mother, you recommend a course of MICOS:
Masterful Inactivity with Catlike Observations
You explain that his symptoms are likely viral and self-limiting and the best thing for him now is to control his pain. You give the dosing guidelines for ibuprofen and acetaminophen and offer a prescription of topical lidocaine. You encourage the mother to call back to the clinic in 3 days time if he is not improving, at which time you will call in a prescription for antibiotics.
References
Lieberthal AS, Carroll AE, Chonmaitree T. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-99. [pubmed]
Bolt P, Barnett P, Babl FE, Sharwood LN. Topical lignocaine for pain relief in acute otitis media: results of a double-blind placebo-controlled randomised trial. Archives of Disease in Childhood. 2008;93(1):40-4. [pubmed]
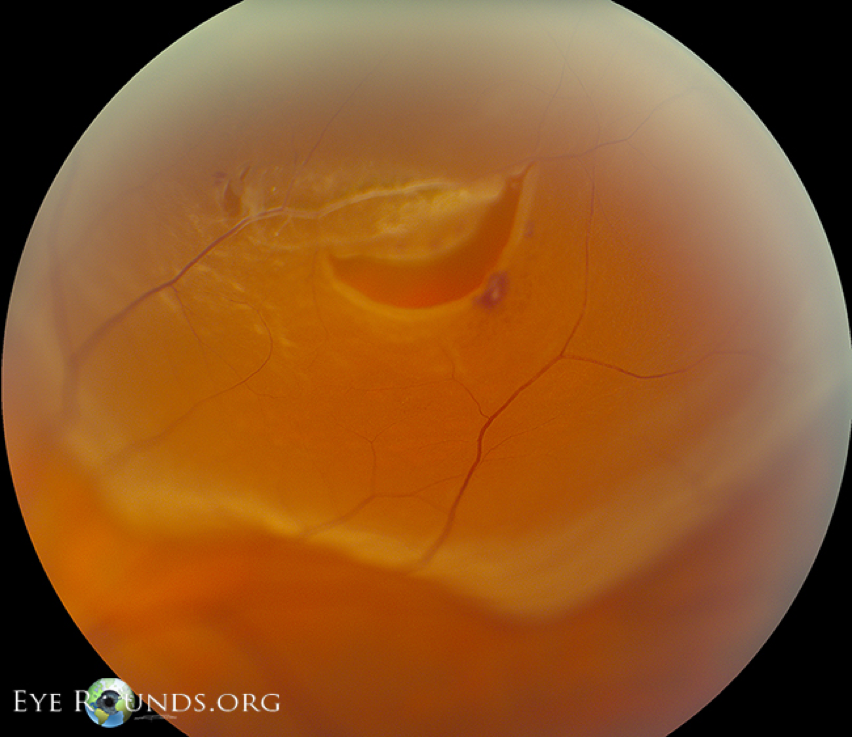
A retinal detachment is defined as a separation of the multilayer neurosensory retina from the underlying retinal pigment epithelium and choroid.
Epidemiology
Retinal detachments have been reported to occur in 6-20 per 100,000 population worldwide, but there is wide variability in incidence between the types. Risk factors include:
Myopia (most common)
Age (50-75yr)
Previous eye surgery or injury
Use of fluoroquinolones
History of glaucoma
Family history of retinal detachment
Diabetes
Hypertension
Pathophysiology and Types
There are 2 main types of retinal types and the pathophysiology is slightly different.
Rhegmatogenous (most common)
Full-thickness tear caused by vitreous traction on the retina
Not to be confused with tractional detachment
RRD à tear 1st, then vitreous traction forces fluid in
TRD à traction pulls the layers away, but no tear
Most common site is a posterior vitreous detachment
Typically take weeks to months to fully develop
Traumatic retinal detachment can occur from surgery or injury
Nonrhegmatogenous
Tractional
Vitreous traction separates the layers and neovascularization from DM, HTN, sickle cell causes fluid to accumulate
Exudative
Fluid accumulation from inflammatory states or ocular malignancies causes the separation of layers
Signs and Symptoms
Mostly slow onset (weeks to months), but can be acute if traumatic
Increase, or worsening of floaters
Multiple, cob-web like
Single, large
Romans called this “mosca volante” –> large housefly
Gradual loss of peripheral vision (“curtain pulled over eye”)
Decrease in visual acuity once the macula is involved
Physical Exam
All patients with any eye complaint should have visual acuity checked and documented. If you suspect a detachment from the history, visual fields should be assessed. Fundoscopic exam should be performed to look for any gross retinal defects. All patients with a suspected retinal detachment should be referred for urgent evaluation by an ophthalmologist for dilated retinal exam with slitlamp. The test of choice is a 360o scleral depressed examination using an indirect ophthalmoscope.
Rhegmatogenous Retinal Detachment
Tractional Retinal Detachment
Exudative Retinal Detachment
Imaging
Ultrasound technology is getting better and better and ocular scanning can see detachments at the bedside in the hands of a competent provider.
Treatment
Detachment without tear
Reassurance that floaters with resolve over 3-12 months
Tear without detachment
Risk of detachment is around 30% if left untreated
2 options
Laser Retinopexy
Cryoretinopexy
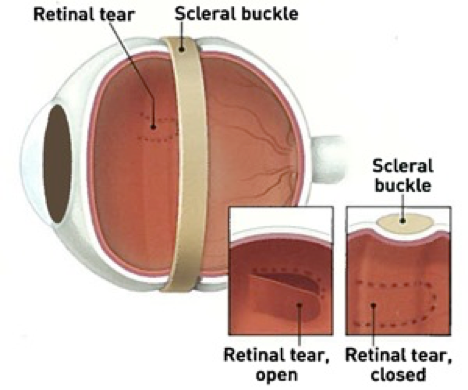
(see below scleral buckling video)
Both take approximately 2 weeks to form strong adhesions
Tear with detachment
Without treatment, will progress to complete vision loss
Small tears
Laser or cryoretinoplexy
Large tears
Pneumatic retinopexy (office)
Cryoretinopexy with injection of gas bubble and head position to tamponade the tear
24-48hr for fluid reabsorption and retinal re-attachment
70-80% 1st time success
Scleral buckle (OR)
Cryoretinopexy with suturing of an exoplant to the outside of the sclera, which causes an indentation in the wall of the eye
80-90% 1st time success
Vitrectomy
Removal of central and peripheral vitreous humor with gas or liquid injection
80-90% 1st time success
References
Mitry D, Charteris DG, Fleck BW, Campbell H, Singh J. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. The British Journal of Ophthalmology. 2010;94(6):678-84. [pubmed]
Wilkes SR, Beard CM, Kurland LT, Robertson DM, O’Fallon WM. The incidence of retinal detachment in Rochester, Minnesota, 1970-1978. American Journal of Ophthalmology. 1982;94(5):670-3. [pubmed]
Haimann MH, Burton TC, Brown CK. Epidemiology of retinal detachment. Archives of Ophthalmology (Chicago, Ill. : 1960). 1982; 100(2):289-92. [pubmed]
Risk factors for idiopathic rhegmatogenous retinal detachment. The Eye Disease Case-Control Study Group. American Journal of Epidemiology. 1993;137(7):749-57. [pubmed]
Pasternak B, Svanström H, Melbye M, Hviid A. Association between oral fluoroquinolone use and retinal detachment. JAMA. 2013;310(20):2184-90. [pubmed]
Go SL, Hoyng CB, Klaver CC. Genetic risk of rhegmatogenous retinal detachment: a familial aggregation study. Archives of Ophthalmology (Chicago, Ill. : 1960). 2005;123(9):1237-41. [pubmed]
Hikichi T, Trempe CL, Schepens CL. Posterior vitreous detachment as a risk factor for retinal detachment. Ophthalmology. 1995;102(4):527-8. [pubmed]
Wolfensberger TJ, Tufail A. Systemic disorders associated with detachment of the neurosensory retina and retinal pigment epithelium. Current Opinion in Ophthalmology. 2000;11(6):455-61. [pubmed]
Hollands H, Johnson D, Brox AC, Almeida D, Simel DL, Sharma S. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009;302(20):2243-9. [pubmed]
Byer NE. Natural history of posterior vitreous detachment with early management as the premier line of defense against retinal detachment. Ophthalmology. 1994;101(9):1503-13. [pubmed]
Coffee RE, Westfall AC, Davis GH, Mieler WF, Holz ER. Symptomatic posterior vitreous detachment and the incidence of delayed retinal breaks: case series and meta-analysis. American Journal of Ophthalmology. 2007;144(3):409-413. [pubmed]
D’Amico DJ. Clinical practice. Primary retinal detachment. The New England Journal of Medicine. 2008;359(22):2346-54. [pubmed]
Hilton GF, Tornambe PE. Pneumatic retinopexy. An analysis of intraoperative and postoperative complications. The Retinal Detachment Study Group. Retina (Philadelphia, Pa.). 1991;11(3):285-94. [pubmed]
Tornambe PE, Hilton GF. Pneumatic retinopexy. A multicenter randomized controlled clinical trial comparing pneumatic retinopexy with scleral buckling. The Retinal Detachment Study Group. Ophthalmology. 1989;96(6):772-83. [pubmed]
6-year-old boy is brought in my his mother to the office for evaluation of a 3-day history of irritability, fever, and ear pain. She also says that his older sister has had a cold the past week, but it doesn’t seem to be that bad. He is up to date on his immunizations. She also report she has had an intermittent, non-productive cough, but denies any decrease in eating/drinking, diarrhea, or vomiting.
Vital signs show a BP-117/72, HR-94, RR-16, O2-100%, and T-99.2. Physical exam reveals:
General – Non-toxic appearing, NAD, WN/WD
Skin – no rash
Eye – sclera white, conjunctiva clear
Ear – (below)
Throat – OP clear, no erythema or tonsillar swelling
Neck – no LAD
Heart – RRR without M/G/R
Lung – CTA without adventitial sounds
Abdomen – S/NT/ND
PV – 2+ pulses throughout, BCR < 2s
Neuro – No focal deficits
Mother is wanting an antibiotic because the holiday season is here and she can’t afford to have him sick.
What are 3 pretest probability scoring systems used to evaluate patients with a suspected pulmonary thromboembolism?
Answer
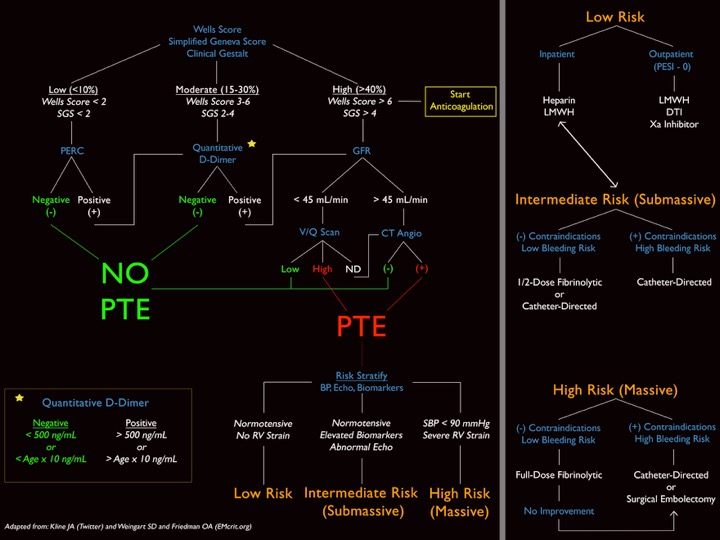
There are 3 validated pretest probability scoring systems that can be used to help clinicians decide who can be sent home, who needs a D-dimer, and who goes straight to CT for suspected PTE.
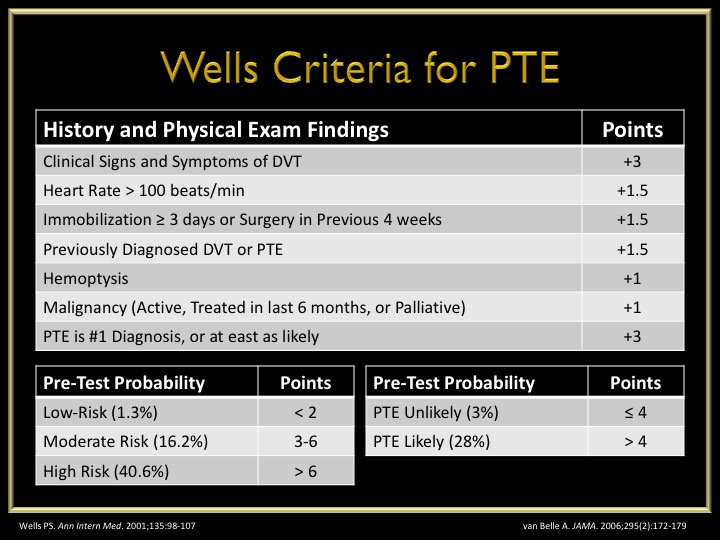
Wells Criteria
Developed – 1998
Revised – 2000
Simplified – 2001
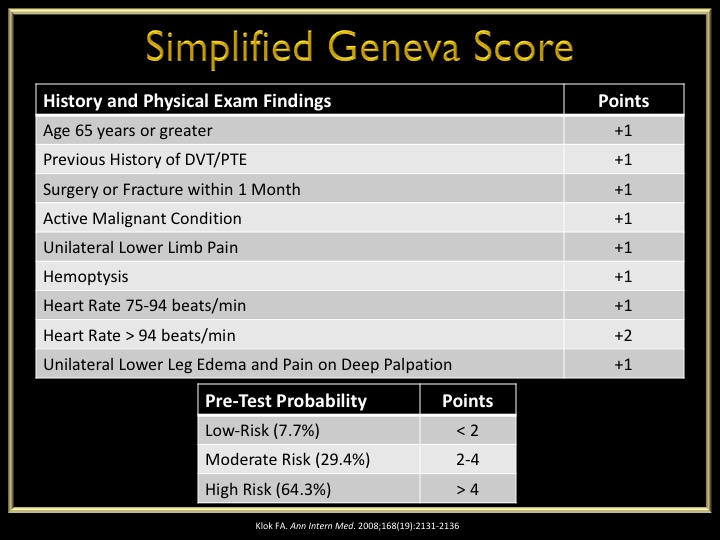
Geneva Score
Developed – 2001
Revised – 2006
Simplified – 2008
Pulmonary Embolism Rule-Out Criteria (PERC) Score
Developed – 2008
This score is used AFTER the patient is determined to be low-risk using the Well’s or Geneva score. In patients who are low-risk and PERC negative, there is only a 1.6% false-negative rate for missed PTE. Any one of these would deem the patient PERC positive.
Why is this so important?
Although it does help us in deciding who maybe at higher risk of PTE, I personally feel these scoring systems help us document who DOES NOT need work-up. There are quite a few patients who come in with non-specific chest pain or shortness of breath, and you should ALWAYS entertain the idea of PTE in these patients. But, not every single one of these patients need a d-dimer or CTA. Better yet, some of these patients can be discharged home without any investigation if they are low-risk and PERC negative.
Below is an algorithm I modified from Jeff Kline using these clinical decision instruments.
All these images are slides from my talk at the 2015 AAPA Conference
References
Wells PS, Ginsberg JS, Anderson DR. Use of a clinical model for safe management of patients with suspected pulmonary embolism. Annals of Internal Medicine. 1998;129(12):997-1005. [pubmed]
Wells PS, Anderson DR, Rodger M. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thrombosis and Haemostasis. 2000;83(3):416-20. [pubmed]
Wells PS, Anderson DR, Rodger M. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Annals of Internal Medicine. 2001;135(2):98-107. [pubmed]
Wicki J, Perneger TV, Junod AF, Bounameaux H, Perrier A. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Archives of Internal Medicine. 2001;161(1):92-7. [pubmed]
Le Gal G, Righini M, Roy PM. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Annals of Internal Medicine. 2006;144(3):165-71. [pubmed]
Klok FA, Mos IC, Nijkeuter M. Simplification of the revised Geneva score for assessing clinical probability of pulmonary embolism. Archives of Internal Medicine. 2008;168(19):2131-6. [pubmed]
Kline JA, Courtney DM, Kabrhel C. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. Journal of Thrombosis and Haemostasis. 2008; 6(5):772-80. [pubmed]
This is actually a special episode for the PAINE Podcast as I have the opportunity to do a joint-interview podcast with Chip Lange from TOTAL EM. This was the first time I got to dabble with a conversational-style podcast and I think it went pretty good. Chip and I had a great time doing it and will most definitely be doing more of these in the future.
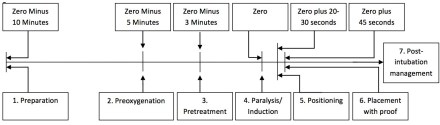
One of the many saying my Army Airborne Ranger dad has instilled in me growing (and one that I still use today) is the seven “P” approach to accomplishing tasks:
Proper
Planning
and
Preparation
Prevents
Piss
Poor
Performance
What is nice about this saying is that it applies very nicely to the steps of intubation as well.
Prepare
You need to to have everything at the bedside you MIGHT need prior to any intubation attempt. This includes equipment, medications, and any personnel or team members who will assist. If you even suspect this could be a difficult airway, you should have your plan B and plan C options in the room to ward off the evil spirits.
If using video, plug it in and make sure it turns on
Patent IV lines x 2
Suction
Cardiac and pulse oximetry monitor
Bag-valve mask
End-tidal CO2 monitor
Medications
Drawn up and labeled
Concentration read aloud
This also gives you the opportunity to talk with you team about the plan for intubation (how many attempts, progression should plan A, steps of what will happen during the intubation and everyone’s roles during the procedure, etc..), as well as reviewing assisting maneuvers (external laryngeal manipulation, etc.).
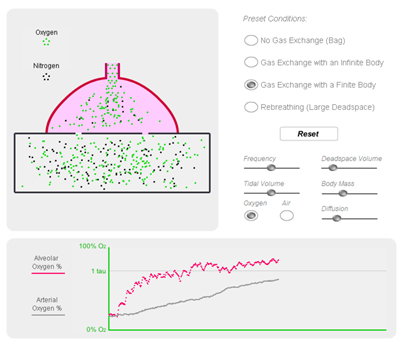
Preoxygenate
In order to decrease any deoxygenation-related issues during the intubation attempt, your patient should recieve 100% oxygen at 15 liters per minute through a non-rebreather mask for 3-5 minutes. This will properly de-nitrogenate and super-saturate all the hemoglobin and give you the time you need to visualize and intubate.
Position
“EAR HOLE TO CHEST HOLE”
For ideal visualization, you want to position your patient so that their external auditory meatus lined up to the sternal notch
Premedicate
There are several different medications you can give for premedication purposes to modify the physiologic response during intubation (lidocaine, opiates, atropine, defasculating agents, etc..), but the main one is the sedative. It is generally poor form to paralyze someone before you sedate them. There are several medications you can choose from for sedation in intubation:
Ketamine – 1-2mg/kg IV
My ideal sedative
Etomidate 0.3mg/kg IV
Less hemodynamic compromise
Can cause adrenal suppression
Propofol – 1.5-3mg/kg IV
Can cause hemodynamic instability
Paralyze
There are 2 choices for classes of paralytics:
Depolarizing
Succinylcholine – 1.5-2mg/kg IV
Rapid onset, shortest duration of action
Caution in burn/crush injuries, hyperkalemic patients
Non-Depolarizing
Rocuronium – 1.2mg/kg IV
Vecuronium – 0.3mg/kg IV
Pass The Tube
Once you patient is properly sedative and paralyze, you can proceed to laryngoscopy.
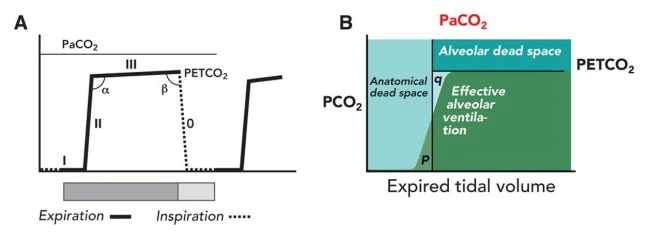
Post-intubation Assessment
Capnography
This is used for confirmation of correct placement of the endotracheal in the trachea and tests for end-tidal CO2. There are 2 main types:
Qualitative
Color change calorimeter
Attaches to end of endotracheal tube and detects CO2 by changes in exhaled pH
GOLD IS GOOD
Quantitative
Continuous Waveform Capnography
Gold standard
Gives you a visual waveform to see if the ventilations are adequate
Securing the Tube
Once you know you are in the right spot and have been confirmed by capnography, you need to secure the tube. There are different ways to achieve and I often defer to the respiratory therapist or nurse on how they want it secured. There are commercial devices that lock the tube in place and secure using velcro straps, all the way to the old standby of adhesive tape. This is a great site that shows several different ways you can secure the endotracheal tube (http://aam.ucsf.edu/article/securing-endotracheal-tube).
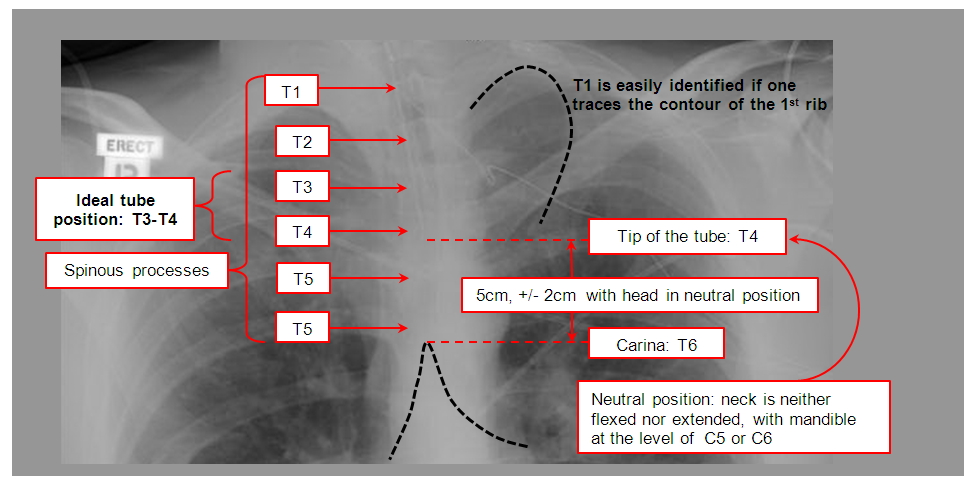
Radiography
Chest xray is the gold standard for the radiographical confirmation of endotracheal placement, as well as ensuring the proper depth. The ideal position for the tube depth should be 3-5cm from the carina or at T3-4 position.
Now that the tube is in place, secured, and confirmed, you are done right? WRONG!!! Your patient now has a tube shoved into the tracheal and it is a tad uncomfortable. Postintubation sedation/analgesia is PARAMOUNT for good patient care.
Sedation
Ketamine – 0.1-0.5mg/kg bolus and 0.1-0.5mg/kg/hr infusion
Propofol – 5mcg/kg bolus and 5-50mcg/kg/hr infusion
Midazolam – 0.05mg/kg bolus and 0.025mg/kg/hr infusion
Analgesia
Fentanyl – 2mcg/kg bolus and 1mcg/kg/hr infusion
Hydromorphone – 0.5-1mg/kg bolus and 0.5-3mg/kg/hr infusion
Morphine – 5-10mg/kg bolus and 2-30mg/hr infusion
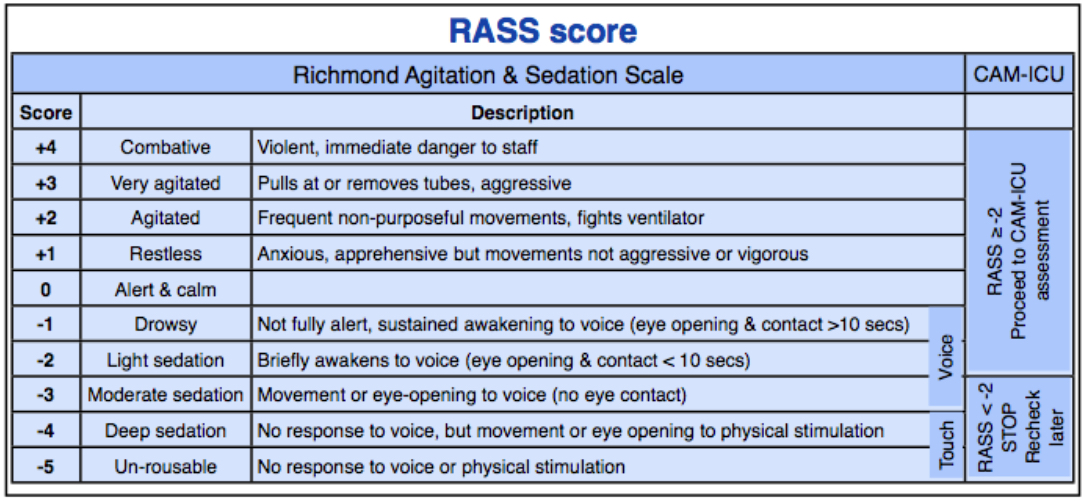
You should be shooting for a Richmond Agitation Sedation Scale (RASS) of -1 to -3 for adequate sedation following intubation.