A large part of critical care and ICU management revolves around hemodynamic monitoring and support. But…..we typically don’t use traditional blood pressure (systolic and diastolic) numbers directly.
We use MAP!!!
What is MAP?
How do you calculate it?
Why is it a better variable to monitor when it comes to blood pressure and critical care?
Definition – intravenous catheter that is maneuvered through the right side of the heart into the pulmonary artery.
Clinical Significance – This catheter can directly measure several important hemodynamic variables in critical illness:
right atrial pressures
right ventricular pressures
pulmonary artery pressures
left atrial filling pressures (wedge pressure)
cardiac output/cardiac index
systemic vascular resistance
pulmonary vascular resistance
It is “floated” through the right side of the heart using the flow of the blood to carry it into the pulmonary artery. This migration has a very characteristic pressure pattern to know where the catheter is in the vascular system.
History – Named after two physicians from Cedars-Sinai Medical Center, Jeremy Swan (1922-2005), an Irish American cardiologist, and William Ganz (1919-2009), a Slovak American cardiologist. Dr. Swan received his medical doctorate from Castleknock College and went on to become faculty at the Mayo Clinic before joining the faculty at Cedars-Sinai Hospital in Los Angeles. Dr. Ganz attended Charles University School of Medicine in Prague in 1938, but was closed in 1940 after the Nazi occupation of Czechoslovakia. Being jewish, he was then sent to a Hungarian Nazi labor camp and was actually scheduled to be sent to Auschwitz in 19944 before his escape. After hiding and waiting out the war, Dr. Ganz returned and graduated from Charles University in 1947 at the top of his class. He practiced in communist Czechslovakia until 1966 when he secretly defected to the US with his wife and sons. His first and only position as a physician in the US was at Cedars-Sinai Hospital, where he met Dr. Swan who got the idea of the catheter from watching the wind play with the sails of boats in the marina. Dr. Ganz had already published research on the use of thermodilution as a way to measure cardiac output and in 1970, they published their landmark article in the NEJM. It should be noted that German surgeon Werner Forssmann first demonstrated the safety of this type of catheter, by doing it on himself in 1929.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Swan HJ, Ganz W, Forrester J, Marcus H, Diamond G, Chonette D. Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter. The New England journal of medicine. 1970; 283(9):447-51. [pubmed]
FRONEK A, GANZ V. [Local thermodilution method of measuring minute volume and circulation rate in the peripheral vessels]. Ceskoslovenska fysiologie. 1959; 8(3):189. [pubmed]
W. Forssmann. Die Sondierung des Rechten Herzens. Klinische Wochenschrift, Berlin, 1929, 8: 2085.
These
studies are conducted at the Ottawa Hospital Research Institute and University
of Ottawa starting in 1992 and the main researcher behind these is Ian Stiell.
They
are international recognized and have been validated multiple times to decrease
unnecessary radiographic testing and decrease healthcare costs
Disclaimer for Using Clinical Decision Instruments
Your
clinical judgement should ALWAYS trump using any CDI
Distracting
injuries
Intoxication
Inability
to fully examine
Gestalt
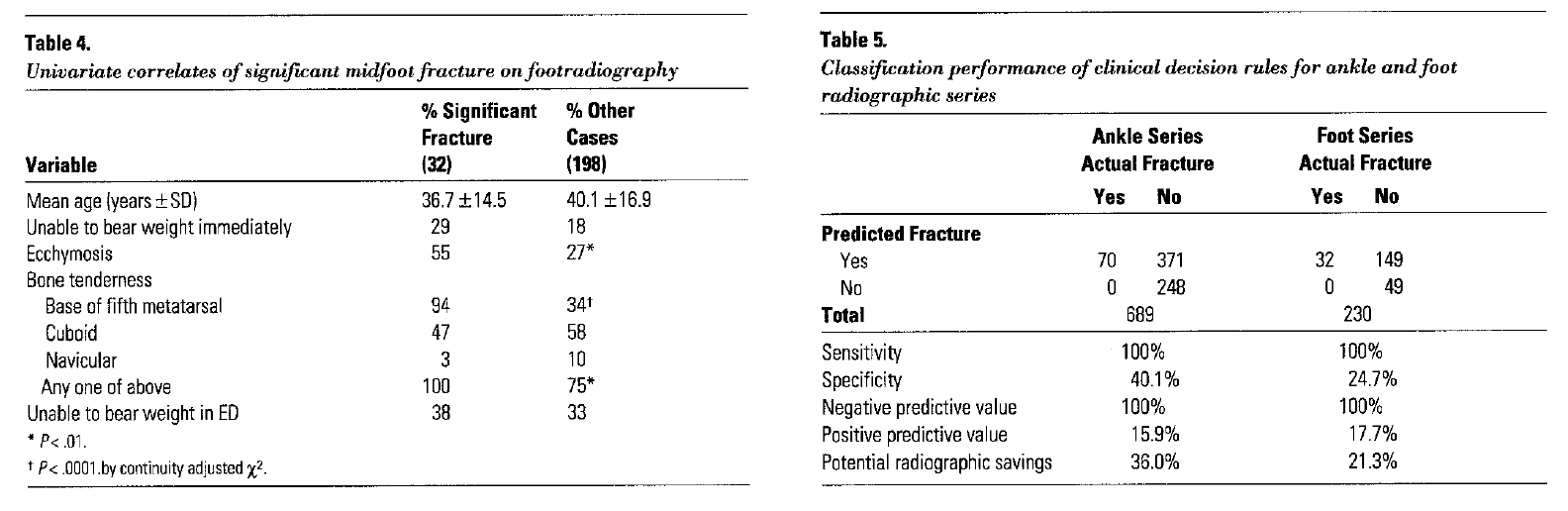
Ottawa Rules of the Foot and Ankle
The
Numbers
Ankle
xrays are the second most commonly ordered film in the ED
<
15% fracture incidence rate
The
study
Published
in 1992, validated in 1995
7
months long
750
patients
21
EM physicians looking at 32 clinical variables
Variables
Lateral
malleolus tenderness
Medial
malleolus tenderness
Base
of 5th metatarsal tenderness
Navicular
tenderness
Inability
to bear weight immediately and in the emergency department for four steps
Limping
counts
Outcomes
Identified
100% of clinically significant fractures
Decreased
ankle imaging 36% and foot imaging 21%
Clinical
Pearls
Be
sure to palpate the entire 6cm of the distal tibia and fibula
Do
not confuse soft tissue tenderness for bony tenderness
Ottawa Rules of the Knee
The
Numbers
>600,000
patients annually present to ED with knee complaints
80%
of these patients have radiography
Majority
have soft tissue injuries
The
study
Published
in 1995, validated in 1996
14
months long
1,047
patients
33
EM physicians looking at 23 clinical variables
Variables
>
55 years of age
Isolated
patella tenderness
Fibular
head tenderness
Inability
to flex knee to 90o
Inability
to bear weight immediately and in the emergency department for four steps
Limping
counts
Outcomes
Identified
100% of clinically significant fractures
Decreased
knee imaging by 28%
Clinical
Pearls
Use
only for injuries < 7 days old
Patella
tenderness only significant if an isolated finding
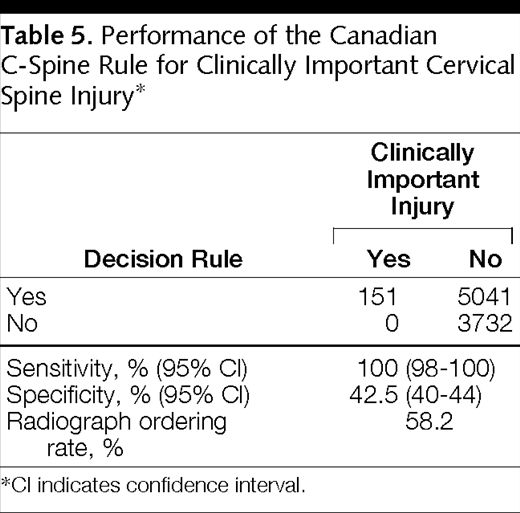
Ottawa Rules of the Cervical Spine
The
Numbers
C-spine
series is the most common radiograph for trauma
>
1,000,000 series performed annually
>
98% being negative
The
study
Published
in 2001, validated in 2003
3
years long
8,924
patients
Blunt
trauma only
Stable
vital signs
GCS
of 15
Looked
at 20 clinical variables
Variables
≥ 65 years of age
Dangerous
mechanism
Fall from height
> 3 feet or 5 stairs
Axial load
High speed (>
60mph) MVC, rollover, or ejection
Motorized
recreational vehicle accident
Pedestrian or
cyclist versus automobile accident
Immediate pain
Non-ambulatory at
scene
Inability to
rotate neck
Outcomes
Identified
100% of clinically significant fractures
Decreased
cervical spine imaging by 42%
Clinical
Pearls
Not
applicable if:
Non-trauma
GCS
< 15
Unstable
vital signs
Age
< 16 years of age
Acute
paralysis
Known
vertebral disease
Previous
cervical spine history
Canadian Head CT Rule
The
Numbers
>
2 million ED visits annually for minor head trauma
Average
cost of CT scan ~ $1200
Average
annual cost > $900 million
<
3% incidence of clinically significant intracranial injuries
The
study
Published
in 2001, validated in 2005
3
years long
3,121
patients
Blunt
trauma only
GCS
between 13-15
<
24 hours on presentations
Must
have loss of consciousness, altered mental status, or amnesia
Across
10 academic hospitals
Looked
at 22 clinical variables
Variables
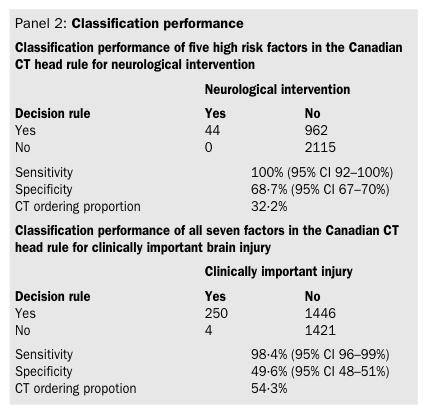
High risk variables (need for neurosurgical intervention)
GCS < 15 at 2 hour after injury
Suspected open/depressed skull fracture
Signs of basilar skull fracture
≥ 2 episodes of vomiting
≥ 65 years of age
Variables
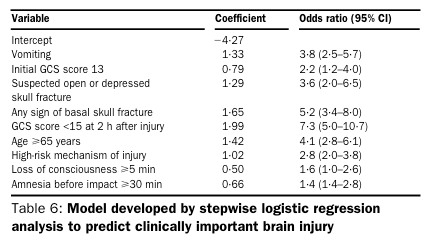
Medium risk variables (predicting clinically important brain injury)
Retrograde amnesia ≥ 30 minutes
Dangerous mechanism
Pedestrian versus auto
MVC ejection
Fall from height > 3 feet or > 5 stairs
Outcomes
Identified
100% of high risk patients and 98.4% of medium risk patients
Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR. A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Annals of emergency medicine. 1992; 21(4):384-90. [pubmed]
Stiell IG, Greenberg GH, McKnight RD, et al. Decision rules for the use of radiography in acute ankle injuries. Refinement and prospective validation. JAMA. 1993; 269(9):1127-32. [pubmed]
Stiell IG, McKnight RD, Greenberg GH, et al. Implementation of the Ottawa ankle rules. JAMA. 1994; 271(11):827-32. [pubmed]
Stiell I, Wells G, Laupacis A, et al. Multicentre trial to introduce the Ottawa ankle rules for use of radiography in acute ankle injuries. Multicentre Ankle Rule Study Group. BMJ (Clinical research ed.). 1995; 311(7005):594-7. [pubmed]
Stiell IG, Greenberg GH, Wells GA, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Annals of emergency medicine. 1995; 26(4):405-13. [pubmed]
Stiell IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA. 1996; 275(8):611-5. [pubmed]
Stiell IG, Wells GA, Hoag RH, et al. Implementation of the Ottawa Knee Rule for the use of radiography in acute knee injuries. JAMA. 1997; 278(23):2075-9. [pubmed]
Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001; 286(15):1841-8. [pubmed]
Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. The New England journal of medicine. 2003; 349(26):2510-8. [pubmed]
Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet (London, England). 2001; 357(9266):1391-6. [pubmed]
Stiell IG, Clement CM, Rowe BH, et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA. 2005; 294(12):1511-8. [pubmed]
Perry JJ, Stiell IG, Sivilotti ML, et al. High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study. BMJ (Clinical research ed.). 2010; 341:c5204. [pubmed]
Perry JJ, Stiell IG, Sivilotti ML, et al. Clinical decision rules to rule out subarachnoid hemorrhage for acute headache. JAMA. 2013; 310(12):1248-55. [pubmed]
You are winding down your 8a-8p shift in the fast track section of your emergency department when a 19-month girl is brought in my her father after falling out of a shopping cart at Home Depot at around 7:15pm. Her father saw her fall and couldn’t catch her before she hit the ground. She immediately began crying and her father denies any loss of consciousness or vomiting. She cried for approximately 30 minutes and her father started to worry that she is now “sleepy”. Other than the sleepiness, her behavior has been normal per her father.
Physical examination does not reveal any periorbital or posterior auricular ecchymosis and there is no hemotympanum. There are no other abrasions or ecchymosis present and her eyes are open and she can track your movements. There is no palpable depressions or crepitus on the skull. She is moving all extremities, reaching for her toys, and saying “Daddy” towards her father.
Does this child need further imaging?
What studies are available to help make this decision?
Answer
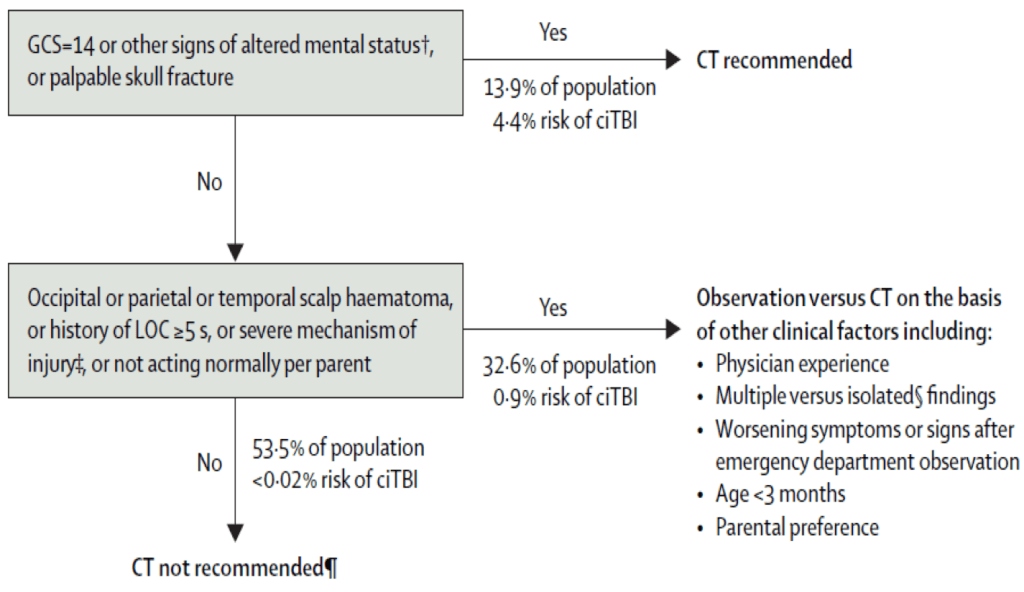
This simple and most evidence-based answer is no…..not according to PECARN. The Pediatric Emergency Care Applied Research Network study of 2009 evaluated over 40,000 children of various ages to determine high yield clinical findings that best predicted clinically important traumatic brain injury on CT scan. The original negative predictive value in children under 2 with the following findings was 100%:
Normal mental status
No scalp hematoma (except frontal)
No loss of consciousness, or < 5 seconds
Non-severe mechanism of injury
No palpable skull fractures
Acting normal per parents
In our patient, you could make the argument to observe in the emergency department as she is “sleepy”, but it is close to bedtime and I would use shared decision making with the father to decide on discharge with good instructions vs observation for 4-6 hours.
References
Kuppermann N, Holmes JF, Dayan PS, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet (London, England). 2009; 374(9696):1160-70. [pubmed]
Schonfeld D, Bressan S, Da Dalt L, Henien MN, Winnett JA, Nigrovic LE. Pediatric Emergency Care Applied Research Network head injury clinical prediction rules are reliable in practice. Archives of disease in childhood. 2014; 99(5):427-31. [pubmed]
Babl FE, Lyttle MD, Bressan S, et al. A prospective observational study to assess the diagnostic accuracy of clinical decision rules for children presenting to emergency departments after head injuries (protocol): the Australasian Paediatric Head Injury Rules Study (APHIRST). BMC pediatrics. 2014; 14:148. [pubmed]
Other Known Aliases – J-wave, camel-hump, hypothermic hump
Definition – positive deflection occurring at the junction between the QRS complex and ST segment, commonly referred to as the J point
Clinical Significance – Osborn waves are classically seen in hypothermia with a core body temperature < 32°C (90°F), but also can be present in severe hypercalcemia, traumatic brain injury, and pericarditis. It is usually most prominent in the precordial leads.
NEJM. 2015
History – Named after John J. Osborn (1917-2014), who was an American intensivist, and received his medical doctorate from Johns Hopkins University in 1943. He completed a nine-month residency in pediatrics before serving as an Army medical officer in World War II in the Pacific Theatre. He first published his preliminary animal research on hypothermia in 1943 before his military service, and picked it back up after returning stateside. He practiced from New York University to Stanford University and was a founding member of the Society of Critical Care Medicine. His research fostered the initial golden age of intensive care medicine and he worked on heart-lung machine designs, as well as hemodynamic monitoring devices. His eponymous paper was published in 1953 entitled “Experimental hypothermia; respiratory and blood pH changes in relation to cardiac function”
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
OSBORN JJ. Experimental hypothermia; respiratory and blood pH changes in relation to cardiac function. The American journal of physiology. 1953; 175(3):389-98. [pubmed]
Partin C. Profiles in Cardiology: John J Osborn. Clin Cardiol. 1998;21;66-68 [link]
You are winding down your 8a-8p shift in the fast track section of your emergency department when a 19-month girl is brought in my her father after falling out of a shopping cart at Home Depot at around 7:15pm. Her father saw her fall and couldn’t catch her before she hit the ground. She immediately began crying and her father denies any loss of consciousness or vomiting. She cried for approximately 30 minutes and her father started to worry that she is now “sleepy”. Other than the sleepiness, her behavior has been normal per her father.
Physical examination does not reveal any periorbital or posterior auricular ecchymosis and there is no hemotympanum. There are no other abrasions or ecchymosis present and her eyes are open and she can track your movements. There is no palpable depressions or crepitus on the skull. She is moving all extremities, reaching for her toys, and saying “Daddy” towards her father.
Does this child need further imaging?
What studies are available to help make this decision?
Definition – Set of clinical decision instruments to help predict pretest probability in various injuries and need for further radiographical studies
Clinical Significance – There are four Ottawa Rules clinical decision instruments that are currently used:
Knee
Foot and Ankle
Cervical Spine
Head CT in mild head injury
History – Named after The Ottawa Hospital Research Institute and the University of Ottawa over series of publications from 1992-2001. These publications have been validated numerous times and shown to decrease health care costs, unnecessary radiographic studies, and decrease throughput time in the emergency department. The brain behind these studies is Ian Stiell, a Canadian physician researcher who received his medical doctorate from the University of Ontario and completed his residency at McGill University. With over 370 publications to his name, he is a powerhouse in the realm of emergency medicine research.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001; 286(15):1841-8. [pubmed]
Stiell IG, Greenberg GH, Wells GA, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Annals of emergency medicine. 1995; 26(4):405-13. [pubmed]
Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR. A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Annals of emergency medicine. 1992; 21(4):384-90. [pubmed]
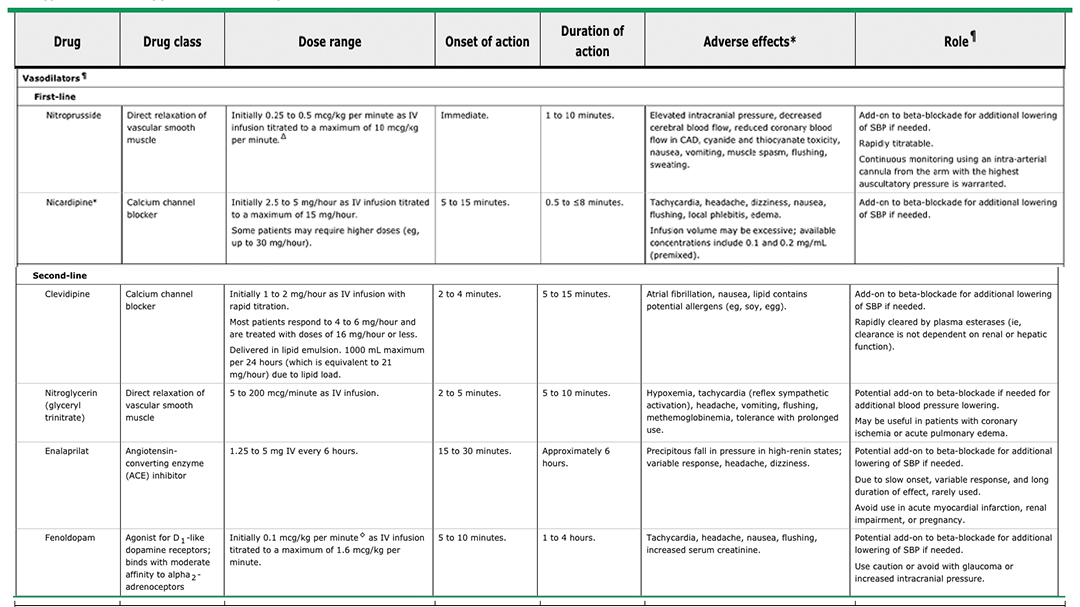
You have a patient in the ED with an aortic dissection and are managing them while awaiting the cardiovascular surgeon to arrive.
What are the two most important things to control?
How do you go about doing that?
Answer
The main aims of acute medical management of aortic dissections are to decrease the rate of left ventricular contraction and decrease the velocity of the contraction, which will overall decrease the shear stress at the site of the tear and slow progression.
Start with intravenous beta-blockade and titrate to a heart rate of 60 betas/minute
If systolic blood pressure is > 120 mmHg after successful beta-blockade, then add a vasodilator or afterload reducer.
Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010; 121(13):e266-369. [pubmed]
Tsai TT, Nienaber CA, Eagle KA. Acute aortic syndromes. Circulation. 2005; 112(24):3802-13. [pubmed]
Wes Johnson, MSPAS, PA-C, (soon to be), DHSc was a former student of mine at UAB and was a respiratory therapist prior to PA school. He is the Regional Director of Clinical Education for Island Medical Management Emergency group in North Alabama. He won the Preceptor of The Year award from UAB in 2016 and currently finishing up his doctorate degree from A.T. Still University.
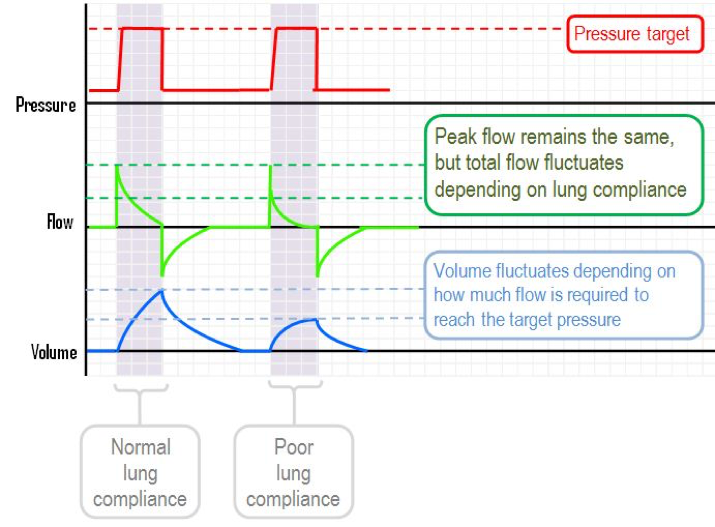
For the purposes of this podcast and post, we will be using the Puritan Bennett 840 ventilator (pictured below). All the term we use are synonymous with all vents, but the screens will be different.
Puritan Bennett 840
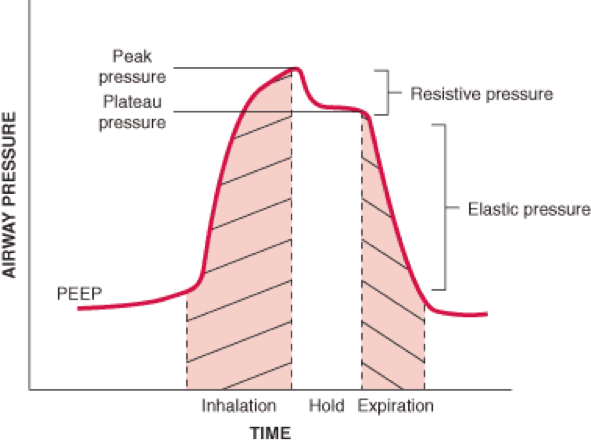
Big Concepts of The Ventilator
Mode
Assist Control (AC)
Every breath is either a machine driven (set by rate) or fully assisted (initiated by the patient)
Tobin MJ. Extubation and the myth of “minimal ventilator settings”. American journal of respiratory and critical care medicine. 2012; 185(4):349-50. [pubmed]